INTRODUCTION
Community – Latinword “COMMUNIS”. A community is a social group determined
by geographical boundaries and / or common values and interests. Its members
know and interact with each other. It functions within a particular structure and
exhibits and creates certain norms, values and social institution.”
Community is a collection of people.
Community is a place.
Community is a social system.
Community is a highly important habitat of man.
Health is related to individual.
But concerned and cooperated effort to people in the community is needed for
individuals health.
3.
DEFINITION :
Community healthnursing is a synthesis of nursing
practice and public practice applied in promoting and preserving
the health of population. The nature of this practice is general
and comprehensive. It is not limited to a particular age or
diagnostic group. It is continuous and not episodic. The dominant
responsibility is to the population as a whole. Therefore, nursing
directed to individuals, families or groups contributes to the
health of the total population. Health promotion, health
maintenance, health education, co-ordination and continuity of
care are utilized in a holistic approach to the management of the
health care of individual, family, group and community. The
nurse’s action acknowledge the need for comprehensive health
planning, recognize the influences of social and ecological
issues, give attention to populations at risk and utilize dynamic
forces which influence change. - ANA
Concepts of communityhealth nursing
Healthful community.
Empowerment for health promotion.
Prevention of premature death Prevention of disease,
illness and disability.
Promotion and maintenance.
Rehabilitation.
6.
PHILOSOPHY OF COMMUNITY
HEALTHNURSING
Philosophy of individual’s right of being healthy.
Philosophy of working together under a
competent leader for the common good.
Philosophy that people in the community have
potential for continued development and are
capable of dealing with their own problems if
educated and helped.
Philosophy of socialism.
7.
OBJECTIVES OF COMMUNITY
HEALTHNURSING
To increase capability of individuals, families,
and groups and community to deal with their
own health and nursing problems.
To strengthen community resources.
To control and counteract environment.
To prevent and control communicable and non-
communicable diseases .
To provide specialized services for mothers,
children, adults, workers, elderly handicapped
and eligible couples etc.
8.
To conductresearch and contribute to the further
refinement and improvement of community health
nursing practice.
To participate in preparing health personnel to
function in community for community health care
services.
To supervise, guide and help health personnel in
carrying out their functions effectively.
9.
PRINCIPLES OF COMMUNITY
HEALTHNURSING
Community health nursing is community
focused, it is therefore essential to know the
defined community, make a map and essential
effective working relationship.
Community health nursing is based on identified,
nursing needs and functions within total
community health programmes.
Health education, guidance and supervision are
integral part of community health nursing
services.
10.
Health servicesshould be realistic in terms of
available resources.
The health worker is responsible to the authorized
health authority and functions within the policies,
general goals and objectives set by the health agency.
Effective health worker irrespective of position or
place of work, functions as a team .
In community health, community is in focus and than
the individual which is the unit of all health care
services .
11.
Professional relationshipsand etiquette are essential
in community health services. Individual and families
participate fully in all decision making relating to
attainment of health.
Continuous services are effective services and
community health nurse must provide continuous
health services.
Well developed system of records and reports is
essential for community health services.
12.
Periodic andcontinuous appraisal and evaluation of
health situation and health services are basic to
community health.
Health services should be available and accessible to all
without any discrimination.
Health worker should be non – political, non-sectarian
in her / his relationship .
Health worker must maintain professional dignity and
must never accept any gift or bribe.
13.
CHARACTERISTICS OF COMMUNITYHEALTH
NURSING
Community health nursing is integral part of community
health.
Community health nursing is a specialized field of nursing.
Community health nursing synthesizes community health
with nursing.
In community health nursing, the whole community is the
client.
Community health nursing emphasizes on primary level
prevention .
Community health nursing promotes self care
responsibility.
Community health nursing involves multidisciplinary team
approach.
14.
Community healthnursing is working for people, with
people and by people.
Community health nursing is seeking support and
giving support to personnel from other sectors working
for welfare and development in the community.
Community health nursing is dealing with wide range
of health problems and health needs and providing
need based generalized health services.
Community health nursing is providing continuous
and not episodic care
15.
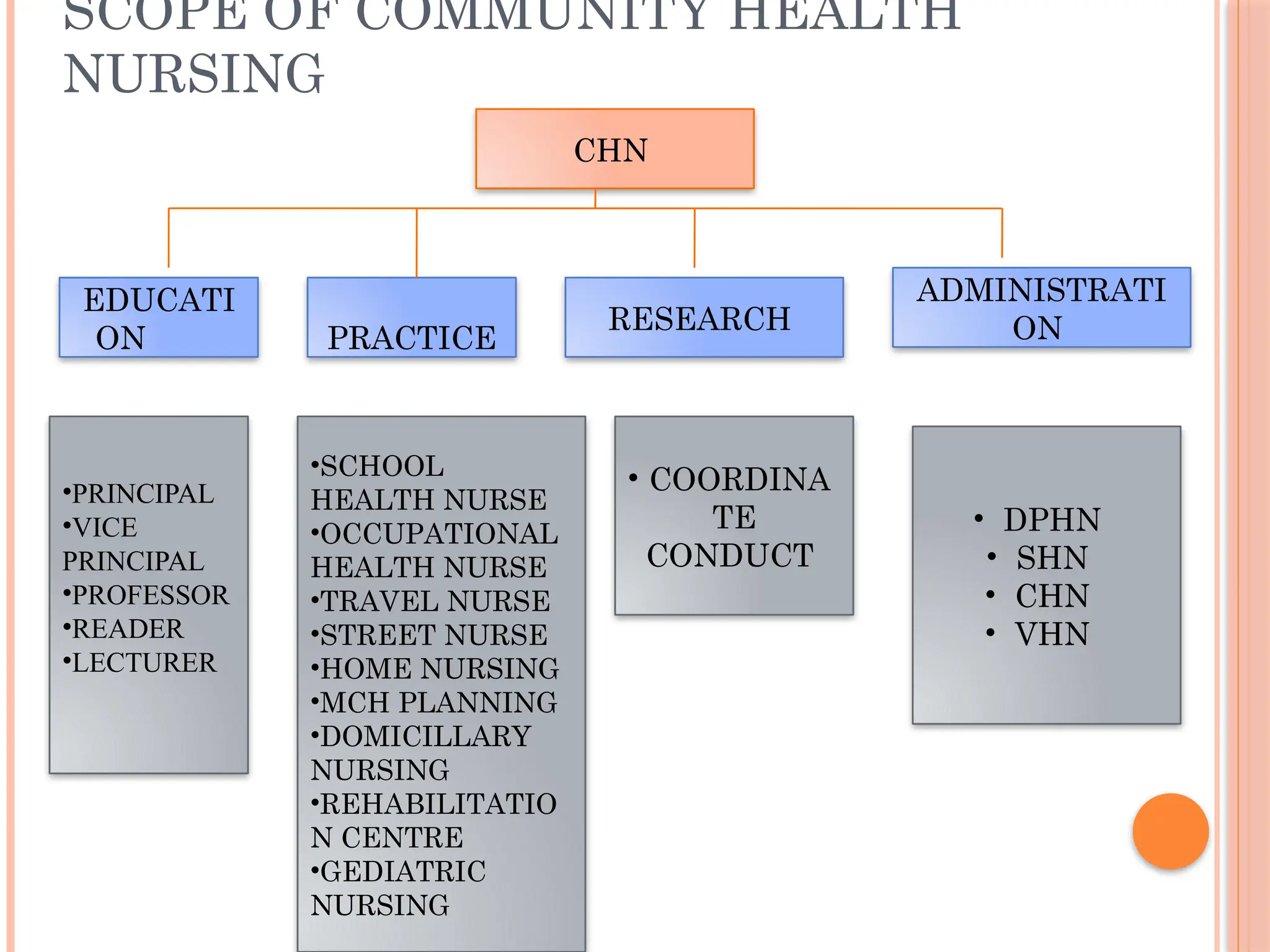
SCOPE OF COMMUNITYHEALTH
NURSING
CHN
EDUCATI
ON PRACTICE
RESEARCH
ADMINISTRATI
ON
•SCHOOL
HEALTH NURSE
•OCCUPATIONAL
HEALTH NURSE
•TRAVEL NURSE
•STREET NURSE
•HOME NURSING
•MCH PLANNING
•DOMICILLARY
NURSING
•REHABILITATIO
N CENTRE
•GEDIATRIC
NURSING
• COORDINA
TE
CONDUCT
• DPHN
• SHN
• CHN
• VHN
•PRINCIPAL
•VICE
PRINCIPAL
•PROFESSOR
•READER
•LECTURER
16.
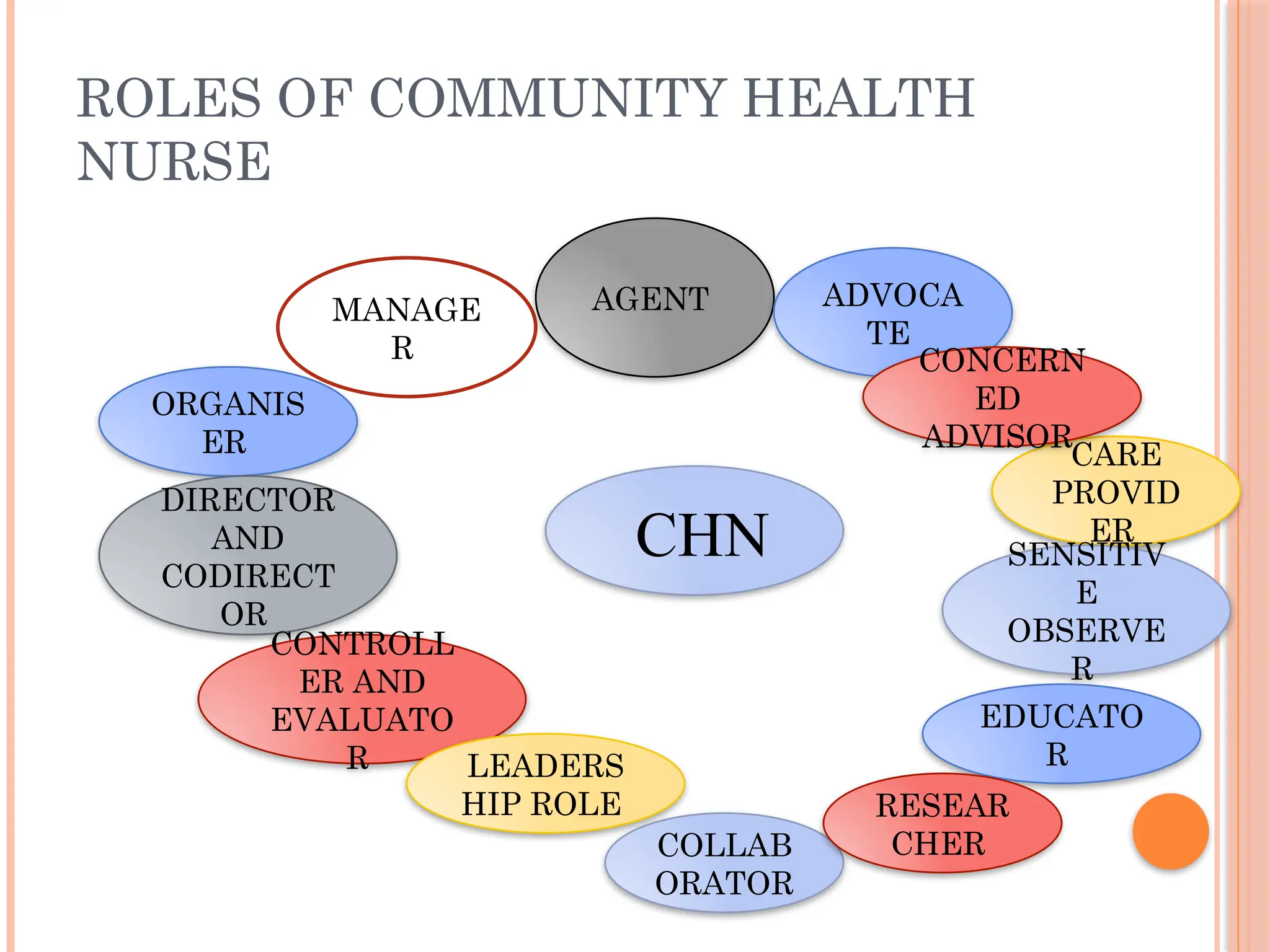
ROLES OF COMMUNITYHEALTH
NURSE
CHN
ORGANIS
ER
MANAGE
R
AGENT ADVOCA
TE
DIRECTOR
AND
CODIRECT
OR
CONTROLL
ER AND
EVALUATO
R LEADERS
HIP ROLE
CARE
PROVID
ER
SENSITIV
E
OBSERVE
R
EDUCATO
R
CONCERN
ED
ADVISOR
COLLAB
ORATOR
RESEAR
CHER
17.
HISTORICAL DEVELOPMENT OF
COMMUNITYHEALTH
Pre – Independence Era:
Early History :
Indus Valley Civilization(before 3,000 B.C) –
planned cities with drainage, houses and public baths
built of backed bricks (Environmental Sanitation)
1400 B.C – Invasion of Aryans. Ayurveda and Siddha
medicine came into existence. Manu Samhita –
prescribed rules and regulations for personal health,
dietetics, hygienic rituals, unity of eh physical, mental
and spiritual aspects of life. Sarve Jana Sukhino Bhavatu
– may all men be free from diseases and may all be
healthy
18.
Post vedicperiod (600 B.C – 600 A.D) – medical education in
University of Taxila and Nalanda leading to the titles of
Pranacharya and Pranavishara . Hospital system was introduced
for men, women and animals by Rahula Sankirtyana .
650 – 1850 A.D – Muslim rulers came to India. Arabic system
of medicine ( Unani ) introduced.
Due to political changes the medical education and medical
services became static and ancient universities and hospitals
disappeared
19.
British India
1757– British established their rule. Civil and
military services established.
1825 – Quarantine Act was promulgated.
1859 – Royal commission was appointed. Pointed out
the need for the protection of water supplies,
construction of drains and prevention of epidemics .
Established “Commission of Public Health.”
1864 – sanitary commission was appointed in Madras,
Bombay & Bengal.
20.
1869 –Public Health Commissioner & Statistical
Officer appointed.
1873 – Birth and Death Registration Act was
promulgated.
1880 – Vaccination Act was passed.
1881 – Indian Factories Act was passed. First Indian
census was taken.
1885 – Local Self Government Act was passed. Local
government came into existence.
1888 – local bodies was directed to look for sanitation
but no local public staff appointed.
21.
1896 –severe epidemic of plague occurred in India.
Plague commission was appointed.
1897- Epidemic Disease Act
1904 – plague commission report submitted. It
recommended the reorganization and expansion of
public health department & establishment of
laboratory facilities for production of vaccines and
sera.
1909 – Central Malaria Bureau at Kausali
1911 – Indian Research Fund Association (now called
as ICMR) to promote research.
1912 – Govt. India decided to help the local bodies.
Appointed Deputy Sanitary Commissioners & Health
Officers.
22.
1918 –Lady Reading Health School, Delhi & Nutrition
Research Laboratory, Coonoor was established.
1919 – First step in decentralization of health
administration. Montague – Chelmsford
Constitutional Reforms – transfer of public health,
sanitation and vital statistics under the control of
elected minister.
1920 – 21 – Municipality & Local Board Acts passed
containing legal provisions for advancement of public
health.
23.
1930 – AllIndia Institute of Hygiene and Public Health,
Calcutta established in aid with Rock feller
Foundation. The Child Marriage Restraint Act( Sarda
Act) came into effect. (Girl – 14 yrs and Boys – 18 yrs)
1931 – Maternity and Child Welfare Bureau established
under IRC.
1935 – Government of India Act (1919) revitalized.
Health activities in the country grouped as federal,
concurrent, provincial.
1937 – Central Advisory Board of Health was set up
with Public Health Commissioner as Secretary and
representatives from provinces and Indian states as
members.
24.
1939 – MadrasPublic Health Act was passed. First Rural Health
training Centre was established at Singur with the aid from
Rockefeller Foundation. Tuberculosis Association of India was
established.
1940 – Drugs Act was passed.
1943 – The Health Survey and Development Committee ( Bhore
committee) was appointed – to survey the existing position
with regard to health conditions and health organization.
25.
1946 – Bhorecommittee submitted its report.
It reviewed on the following and recommended short
and long term programme to attain reasonable health.
Public health
Medical relief
Professional education.
Medical research.
International health.
26.
Post independence era:
1947 – Ministries of health established in state &
center. Post of Director General of Health Services
( principal advisor to the union government on both
medical & public health matters) was formed by
combining the posts of Public Health Commissioner&
director general of Indian Medical Service.
1948 – India joined WHO as a member state. ESI Act
passed in 1948. the report of the Environmental
Hygiene Committee was published.
27.
1949 – constituentAssembly adopted the constitution of
India(Article 246 covers all the health subjects). Post of
registrar general of India created in the ministry of
home affairs. SEARO office established in New Delhi.
The Indian Research Fund Association was
reconstituted as ICMR.
1950 – planning commission was set up.
1951 – First five year plan begin. BCG vaccination
programme launched.
1952 – community development block launched. Central
council of health was constituted. Primary health
center was set up.
28.
1953 – NMCPcommenced. National Extension
programme was started for rural development. Nation
wide family programme was started. A committee was
appointed to draft a Model Public Health Act.
1954 – Contributory Health Service Scheme was started
at Delhi. The Central Social Welfare Board was set up.
National water supply & sanitation programme was
inaugurated. NLCP was started. VDRL antigen was set
up in Calcutta. The prevention of Food Adulteration
Act was passed.
29.
1955 –NFCP was commenced. The central leprosy teaching
and research institute established in chengelpet. A filaria
training centre was established at Ernakulum. The Hindu
marriage act passed. National TB sample survey commenced.
1956 – second five year plan launched. The model public
health act published. The central health education bureau was
established. Director, family planning appointed. Demographic
training & research centre established in Bombay. The TB
chemotherapy centre established in Madras. The immoral
traffic act was passed. Trachoma control pilot project was
established. RCA project was established with aid from ford
foundation.
30.
1957 – influenzapandmeic swept the country. The demographic
research centers was established in Calcutta, Delhi & Trivandrum.
1958 – NMCP converted into NMEP. Leprosy Advisory
committee of the Govt. of India was constituted. The National
Development Council endorsed the recommendations made by
Balwantrai Mehta Committee on Panchayth Raj. The national Tb
survey was completed.
1959 – Mudhaliar committee was appointed. Central expert
committee was appointed under ICMR to study the problems of
cholera and chicken pox in India. Rajasthan was first state to
introduce panchayath raj. National TB institute was established at
Bangalore. The national research laboratory at coonoor was
shifted to Hyderabad.
31.
1960 –School Health Committee was constituted. A National
Nutrition Advisory Committee was constituted. Pilot projects for
eradication of small pox was initiated. Vital statistics was
transferred to the Registrar General of India.
1961 – third five year plan launched. The report of Mudhaliar
Committee was published. The Central Bureau of Health
Intelligence was established.
1962 – Central Family Planning Institute was established in
Delhi. National Small Pox Eradication Programme was
launched. The School Health Programme was initiated. National
Goiter Control Programme was launched. The District
Tuberculosis Programme was formulated.
32.
1963 –Applied Nutrition Programme was launched. Defense
Institute of Physiology and Allied Sciences was set up.
National Institute of Communicable Diseases was inaugurated.
National Trachoma Control Programme was launched.
Contributory Health Service Scheme was changed into CGHS.
Extended family planning programme was launched. Chadha
Committee established a norm of one basic health worker for
every 1000 population. A drinkling water board was set up.
1964 – National Institute of Health Administration and
Education was opened in collaboration with Ford foundation.
Committee was set up under the chairmanship of Shanthilal
Shah to study the question for legal abortion.
33.
1965 –lippesloop was recommended as safe.
Reinforced extended family planning was launched.
BCG vaccination on a house to house basis introduced.
1966 – Mukherjee committee was set up. Minister of
health was also appointed for minister of family
planning. A separate department for family planning
was started. The population council started
International postpartum family planning programme.
1967 – Modhok committee was constituted. A small
family norm committee was set up. The central council
of health recommended the levy of a health cess on
patient attending hospital.
34.
1968 –small family committee’s report was submitted. A bill
of registration of birth and death was passed. The govt. of India
appointed medical education committee.
1969 – fourth five year plan launched. The name of the
Nutrition Research Laboratory was changed into National
Institute of Nutrition. Comprehensive legislation for control of
river water pollution was drafted. The central births and deaths
registration act was promulgated. The report of the medical
education committee was submitted.
35.
1970 –The Drugs Order was promulgated. All India Post
Partum Family Planning Programme was started. The
population council of India was formed. Chittaranjan mobile
hospitals was installed. The registration of births and deaths Act
came into force. The name of the Demographic Training and
Research Center, Bombay was changed into International
Institute for Population studies.
1971 – The family pension scheme for industrial workers came
into force. MTP bill passed in parliament. An expert committee
was appointed to draft legislation on air pollution.
36.
1972 –MTP act came into force. National service bill
passed. The National Nutrition Monitoring Bureau
was set up under the ICMR.
1973 – the national programme for minimum needs
was incorporated with the fifth five year plan. The
government envisaged a scheme of setting 30 bedded
rural hospitals one for 4 PHC. Kartar singh committee
submitted its report.
1974 – fifth five year plan launched. Parliament
enacted the Water Act.
37.
1975 –India became small pox free. Govt. of India accepted
NMEP. ESI Act amended. Cigarettes Regulation Act was
passed in parliament. Shrivastav committee submitted its
report.
1976 – Indian Factories Act amended. The prevention of food
adulteration act came into force. The equal remuneration act
was promulgated. New population policy announced. Central
council of health proposed 3 – tier plan for medical care.
National programme for prevention of blindness was
formulated.
38.
1977 –National Institute of Health and Family Planning formed.
Rural health scheme was launched. Revised modified plan of
malaria eradication put into operation.
1978 – child marriage restraint bill approved in parliament. EPI
launched.
1979 – offices of family welfare and NMEP were merged and
named as Regional Office for health and family welfare. 1980 –
sixth five year plan launched. Small pox was officially declared
from entire world.
39.
1981 –census was taken. The Air Act was enacted.
1982 – new 20 point programme was announced. National
health policy announced.
1983 – IMPACT India launched (National Plan of Action
Against Avoidable Disablement). NLCP called as NLEP. Guinea
worm eradication programme launched.
1984 – Bhopal gas tragedy occurred. Workmen’s compensation
act came into force. Juvenile Justice Act came into force.
1985 – seventh five year plan launched. UIP launched. A
separate department of women and child development was set
up.
40.
1986 –The Environment Act promulgated. Mental
health bill was voted in parliament.
1987 – new 20 point programme was launched. ISI
was renamed as Bureau of Indian Standards. Safe
motherhood campaign was launched. National
diabetes control programme and national AIDS control
programme initiated.
1989 – blood safety programme was launched.
1990 – control of ARI programme initiated.
1991 – decadal census was conducted.
41.
1992 – eighthfive year plan was launched. CSSD was launched.
The Infant Milk Substitute, Feeding Bottles and Infant Foods Act
came into force.
1993 – RNTCP with DOTS introduced. National Nutrition policy
formulated.
1994 – Return of plague. Panchayath Raj Act came into force.
1995 –ICDS renamed as IMCD. The Legislation on
Transplantation of Human Organs was enacted. Expert Committee
on Malaria submitted its report and recommended Malaria Action
Plan.
42.
1996 – PPIlaunched. Family planning programme made target
free. PNDT came into force. Yaws eradication programme came
into force.
1997 – RCH launched. Ninth five year plan launched.
1998 – 99 – NFHS II undertaken. NMEP renamed as National Anti
– Malaria Programme.
Phase – II of National Aids Control Programme became effective.
National Policy for Older Persons announced.
43.
2000 –govt. of India announced national population
policy. Declared guinea worm free country. Signatory
of UN millennium declaration. National commission
on population constitute.
2001 – fist census of the century. National policy for
empowerment of women launched.
2002 – National Health Policy announced. Govt.
announced National AIDS Prevention and Control
Policy. Tenth five year plan launched. Emergence of
SARS.
2003 – parliament approves the Cigarette and Tobacco
Products Act. NVBDCP approved.
44.
2004 –Vandematarum scheme launched. Revised programme
of National support to primary education launched. Low
osmolality Ors introduced. IDSP launched. National guidelines
on infant and young child feeding formulated.
2005 – RCH – II launched. JSY launched. NRHM launched.
IPHS for community centres formulated. National plan of
Action for children formulated. India achieved leprosy
elimination target.
45.
2006 –WHO releases pediatric growth chart. Ban on
child labor. RNTCP covers whole country. NFHS – II
conducted. IMNCI launched.
2007 – 11 th five year plan launched. NACP –III
launched. IPHS standards for PHC and sub center
formulated. Maintenance and welfare of parents and
senior citizens bill passed.
2008 – Non communicable diseases programme was
launched.
46.
2009 –H1N1 outbreak. New ICDS mother and child
protection card came into force.
2010 – ICMR announces nutrients requirement for RDA
for Indians.