Downloaded 97 times
![Why Bone Pain Bone pain is the most common symptom in myeloma, affecting nearly 70% of patients. The pain usually involves the back and ribs, and unlike the pain of metastatic carcinoma, which often is worse at night, the pain of myeloma is precipitated by movement. Persistent localized pain in a patient with myeloma usually signifies a pathologic fracture. The bone lesions of myeloma are caused by the proliferation of tumor cells, activation of osteoclasts that destroy bone, and suppression of osteoblasts that form new bone. The osteoclasts respond to osteoclast activating factors (OAF) made by the myeloma cells.[OAF activity can be mediated by several cytokines, including IL-1, lymphotoxin, macrophage inhibitory factor (MIP)-1 , and tumor necrosis factor (TNF)]. However, production of these factors decreases following administration of glucocorticoids or interferon](https://image.slidesharecdn.com/12-multiplemyeloma-111031015909-phpapp01/75/multiple-myeloma-7-2048.jpg)
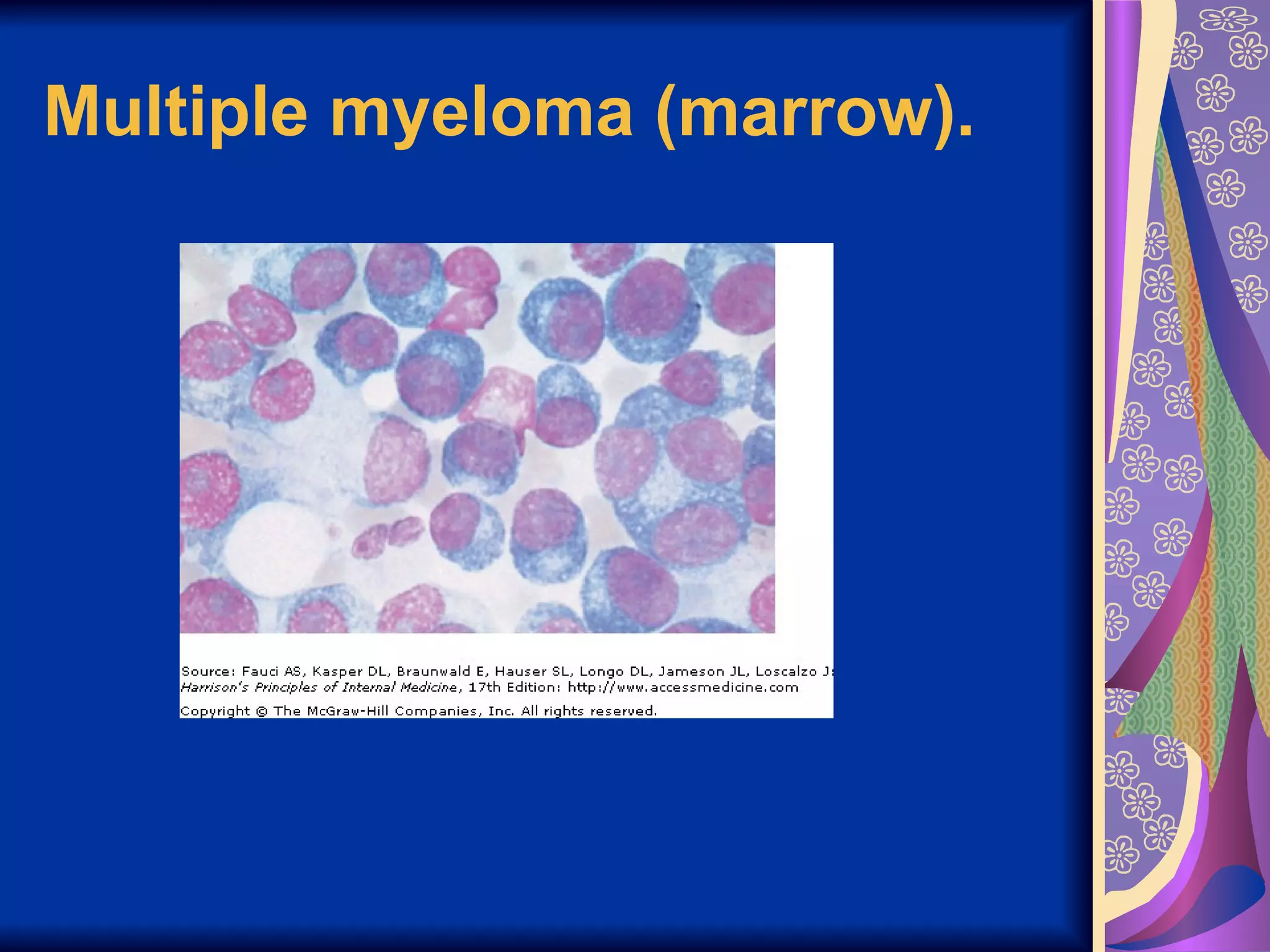

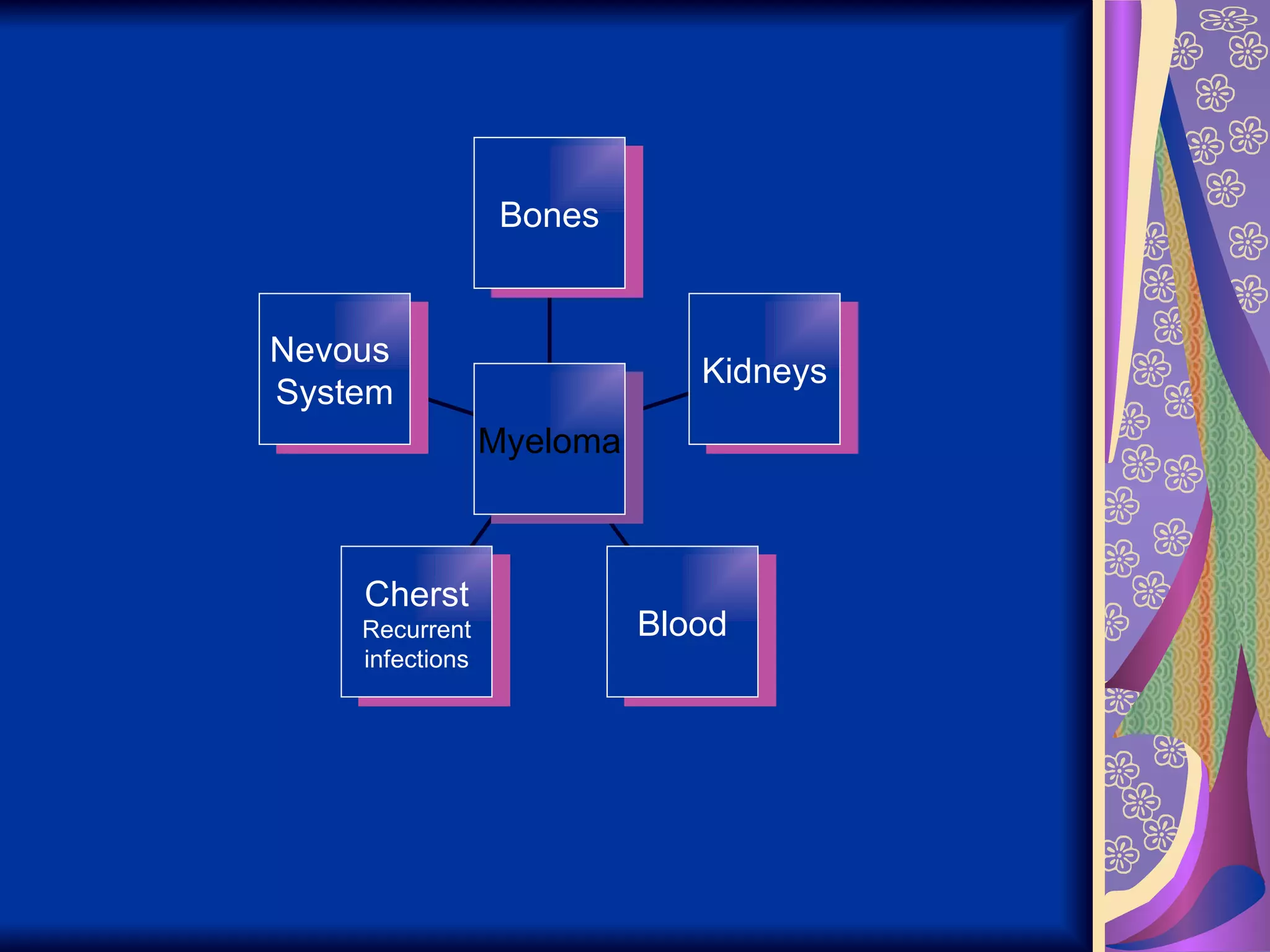
Multiple myeloma is a cancer of plasma cells that results in numerous symptoms. It is caused by malignant proliferation of a single clone of plasma cells in the bone marrow. Symptoms include bone pain, fractures, kidney failure, infections, anemia, high calcium levels, and occasionally blood clotting issues, neurological problems, and hyperviscosity symptoms. Treatment involves chemotherapy and stem cell transplants to control disease progression and manage complications.
Hard work is depicted as the steady path to success, while luck is an uncertain factor.
Multiple myeloma is characterized by malignant plasma cell proliferation with uncertain causes. Associated symptoms include organ dysfunctions and chromosomal alterations.
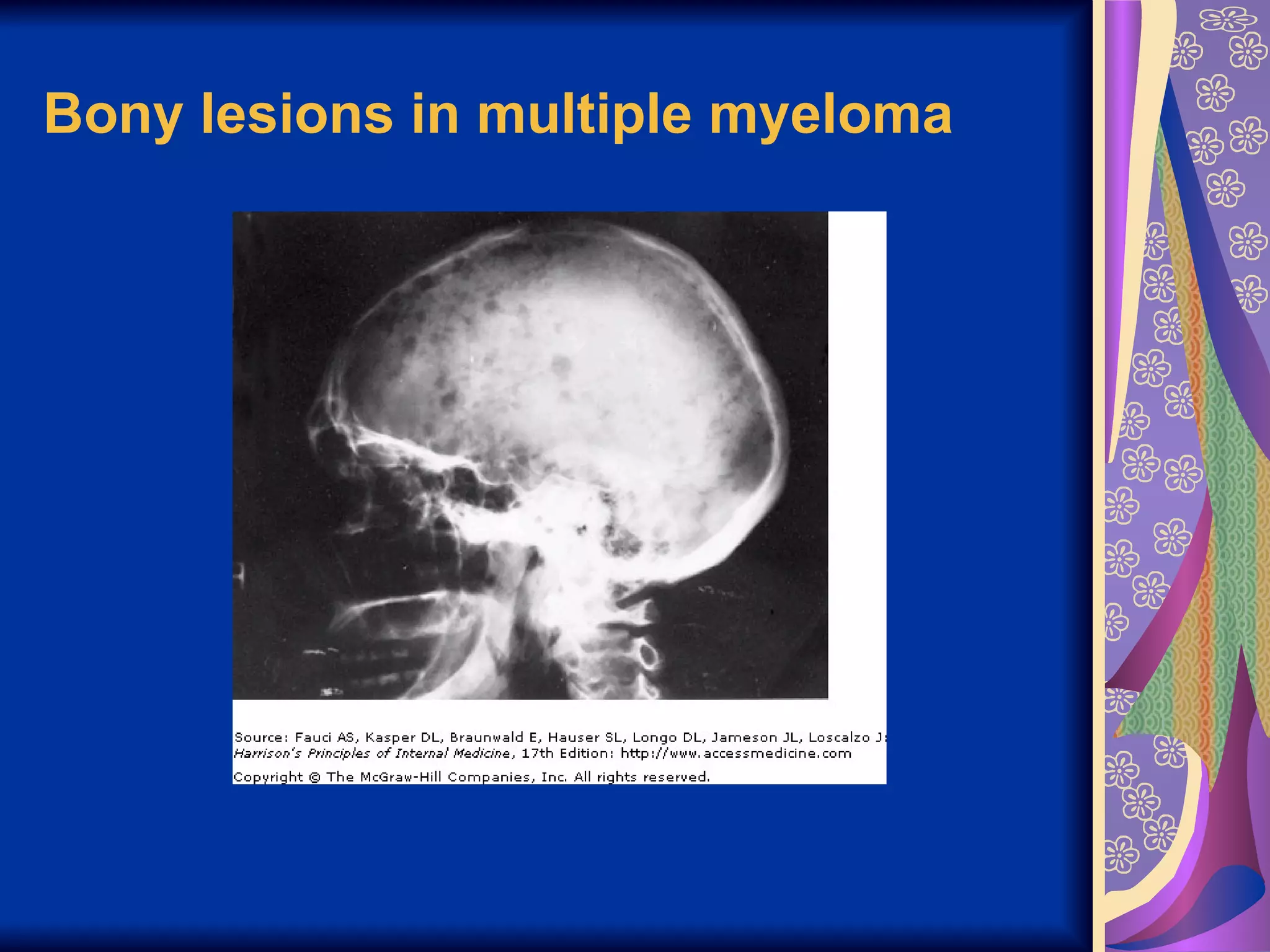
Patients commonly experience symptoms like bone pain, fractures, renal failure, and recurrent infections due to various pathophysiological factors.
POEMS syndrome involves multiple conditions associated with multiple myeloma, highlighting its complexity.
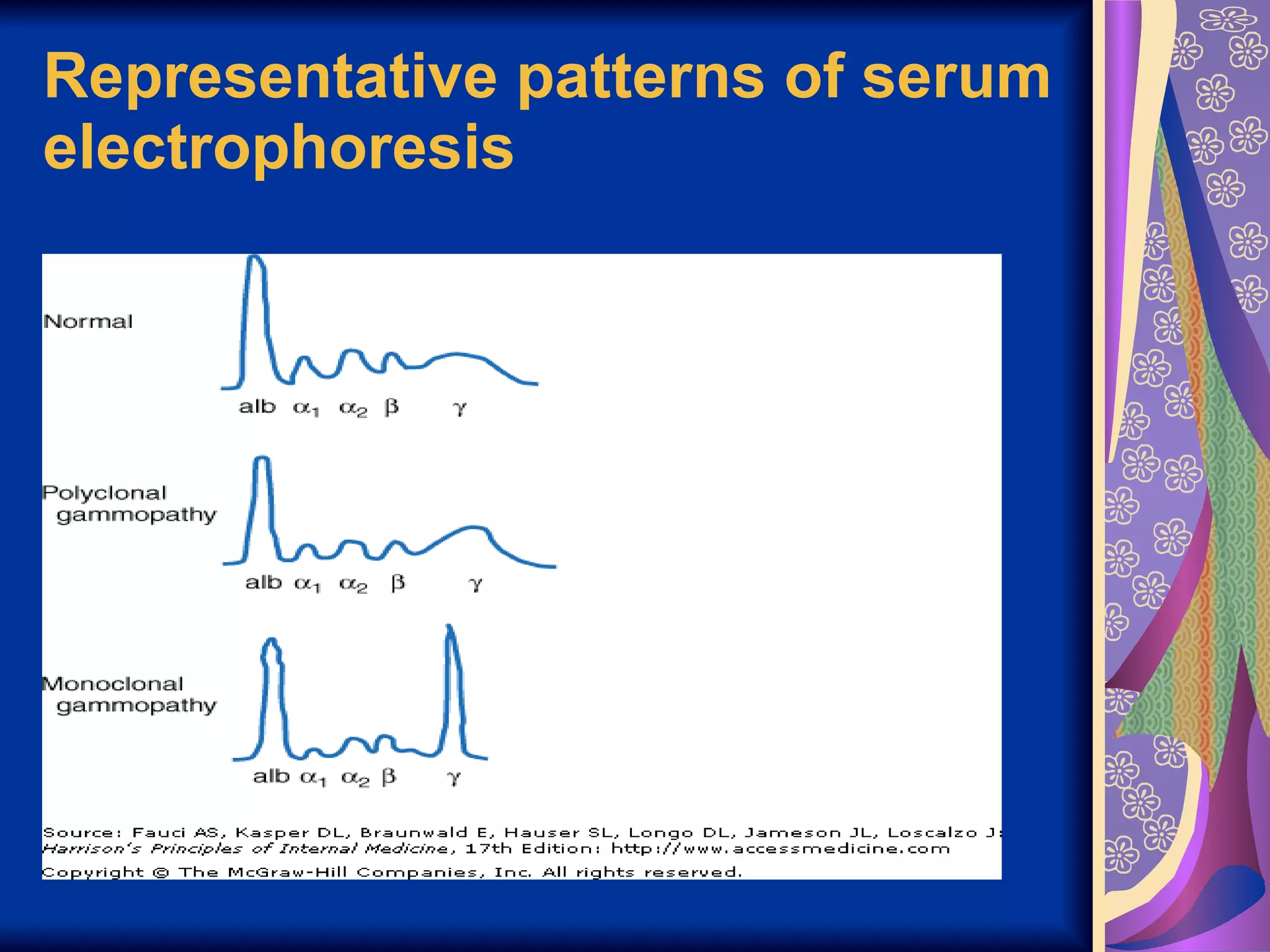
Tests like serum electrophoresis, marrow examination, and imaging help in diagnosing multiple myeloma.
Treatment varies from systemic therapies for symptomatic patients to localized radiation, with survival rates improving through effective interventions.
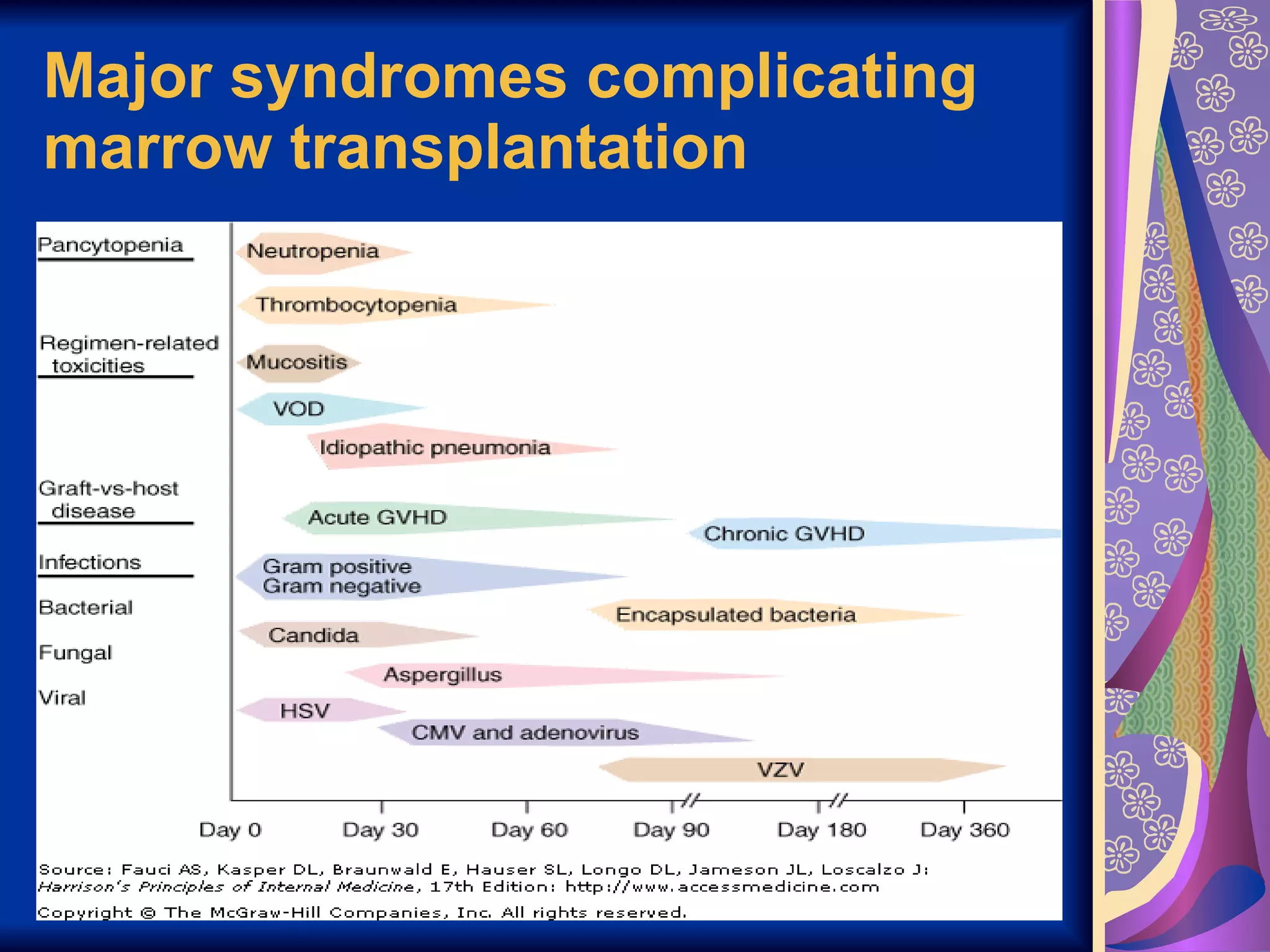
Complications like venoocclusive disease, graft-versus-host disease, and viral infections are significant risks following marrow transplantation.




![Multiple myeloma[1]](https://cdn.slidesharecdn.com/ss_thumbnails/multiplemyeloma1-190414034945-thumbnail.jpg?width=640&height=640&fit=bounds)