Multiple myeloma is a cancer of plasma cells that are found in the bone marrow. It is characterized by an overproduction of abnormal plasma cells which produce a monoclonal protein known as M protein. Symptoms include bone pain or fractures, anemia, kidney problems, and infections. Diagnosis involves blood and urine tests to detect the M protein as well as imaging tests and a bone marrow biopsy. Treatment depends on disease severity and transplant eligibility and may include chemotherapy, steroids, and stem cell transplantation.
MULTIPLE MYELOMA -HEMATOLOGIC MALIGNANCY-DISEASE OF BONE MARROW - PLASMA CELL DISORDER
PATHOLOGY, .CLINICAL FEATURES , AND ITS MANAGMENT REFERENCE HARRISON
MULTIPLE MYELOMA -HEMATOLOGIC MALIGNANCY-DISEASE OF BONE MARROW - PLASMA CELL DISORDER
PATHOLOGY, .CLINICAL FEATURES , AND ITS MANAGMENT REFERENCE HARRISON
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
Plasma cell disorders is a difficult topic where most residents and students confuse with regarding to differentiating between various types of para-proteinemias or plasma cell dyscrasias. This simple presentation will highlight the key points in differentiating, diagnosing these orders. Initial management principles are discussed as well.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
Plasma cell disorders is a difficult topic where most residents and students confuse with regarding to differentiating between various types of para-proteinemias or plasma cell dyscrasias. This simple presentation will highlight the key points in differentiating, diagnosing these orders. Initial management principles are discussed as well.
Multiple myeloma(MM) is hematologic malignancy characterized by neoplastic proliferation of single clone of plasma cell in bone marrow engaged in production of monoclonal (M) protein.
multiple myloma
By: Nader Amir Al-assadi
Supervised by : Dr/ Ghazi Alariqe
taiz university
Multiple myeloma (MM) is a plasma cell malignancy in which monoclonal plasma cells proliferate in bone marrow, resulting in an over abundance of monoclonal para protein (M protein), destruction of bone, and displacement of other hematopoietic cell lines.
The precise etiology of MM has not yet been established.
Roles have been suggested for a variety of factors, including genetic causes, environmental or occupational causes,radiation, chronic inflammation, and infection .
references
20th edition of Harrison's T.B. OF INTERNAL MEDICINE
Blood and Lymphatic Cancer: Targets and Therapy
Advances in the diagnosis and management
of lymphoma
Zachary H Word1
Matthew J Matasar1,2
AML:ACUTE MYELOID LEUKAEMIA
for medical colleges teaching faculty and students as well. it includes AML causes , histopathological slides of subclasses of Acute myeloid leukemia, classification , diagnosis, management modalities, complications .Acute leukemias are stem cell disorders characterized by malignant neoplastic proliferation and accumulation of immature and non functional hematopoietic cells in the bone marrow.
The neoplastic cells show increased proliferation and/or decreased apoptosis.
If the defect primarily affects the common myeloid progenitor (CMP) then it is called Acute myeloid leukemia.
Acute myeloid leukemia (AML) is a neoplastic disease characterized by infiltration of the blood, bone marrow, and other tissues by proliferative, clonal undifferentiated cells of the hematopoietic system.
AML is the result of a sequence of somatic mutations in a multipotential primitive hematopoietic cell or, in some cases, a more differentiated progenitor cell.
It can be slow growing or rapidly fatal.
AML is the predominant form of leukemia during the neonatal period
Incidence : 1.5/100,000/year in infants decreases to approximately 0.4 per 100,000 children ages 5 to 9 years, increases gradually to 1.0 persons per 100,000 until age 25 years, and thereafter increases exponentially until the rate reaches approximately 25/100,000 persons.
AML accounts for 15 to 20 percent of the acute leukemias in children and 80 percent of the acute leukemias in adults.
Men > Women (4.5 : 3)
HEREDITY
1) Chromosomal aneuploidy like Trisomy 21 noted in Down syndrome
2) Defective DNA repair, e.g., Fanconi anemia, Bloom syndrome, and Ataxia telangiectasia
3) Congenital neutropenia ie Kostmann syndrome
4) Germline mutations of CCAAT/enhancer-binding protein α (CEBPA), runt-related transcription factor 1 (RUNX1), and tumor protein p53 (TP53) have also been associated with a higher predisposition to AML
RADIATION
Peaks after 5 to 7 yrs of exposure.
Therapeutic radiation alone seems to add little risk of AML but can increase the risk in people also exposed to alkylating agents.
CHEMICAL AND OTHER EXPOSURES
Exposure to benzene, plastic, rubber, petroleum products, paint, ethylene oxide, herbicides and pesticides can increase the risk.
Smoking can also increase the risk
DRUGS
Anticancer drugs are the leading cause of therapy-associated AML.
Alkylating agent–associated leukemias occur on average 4–6 years after exposure, and affected individuals have aberrations in chromosomes 5 and 7.
Topoisomerase II inhibitor–associated leukemias occur 1–3 years after exposure, and affected individuals often have aberrations involving chromosome 11q23.
Other agents like Chloramphenicol, phenylbutazone, and, less commonly, chloroquine and methoxypsoralen.
SYMPTOMS :
Present with nonspecific symptoms initially.
Fatigue is the first symptom
Fever with or without infection will be present in approximately 10% patients
Bleeding, easy bruising
occasional
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
2. WHAT IS MYELOMA?
Multiple Myeloma (also known as Myeloma or Plasma Cell Myeloma)
is a malignancy of plasma cells, which are the white blood cells
responsible for the production of antibodies (proteins).
MM is characterized by a proliferation of malignant plasma cells and
a subsequent overabundance of monoclonal paraprotein (M protein).
When plasma cells become cancerous and grow out of control, they
can produce a tumor called a plasmacytoma. These tumors generally
develop in a bone, but they are also rarely found in other tissues. If
someone has only a single plasma cell tumor, the disease is called
an isolated (or solitary) plasmacytoma. If someone has more than
one plasmacytoma, they have multiple myeloma.
4. ETIOLOGY
The precise etiology of MM has not yet been established. Roles have
been suggested for a variety of factors, including genetic causes,
environmental or occupational causes, MGUS, radiation, chronic
inflammation, and infection.
.Genetic
.Environmental:agriculture, food, and petrochemical
.MGUS-SMM
.Radiation
.Chronic inflammation
.Infection:Human herpesvirus 8 (HH8) infection of bone marrow
dendritic cells
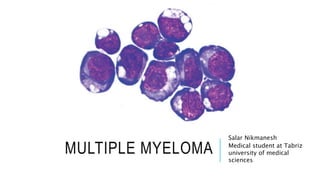
5. PATHOPHYSIOLOGY AND CLINICAL
PRESENTATION
MM is characterized by neoplastic proliferation of plasma cells
involving more than 10% of the bone marrow and overproduction of
monoclonal immunoglobulin G (IgG), immunoglobulin A (IgA), and/or
light chains, which may be identified with serum protein
electrophoresis (SPEP) or urine protein electrophoresis (UPEP). The
pathophysiologic basis for the clinical sequelae of MM involves the
skeletal, hematologic, renal, and nervous systems.
6. 1.SKELETAL PROCESSES
Plasma-cell proliferation causes extensive skeletal destruction with
osteolytic lesions, anemia, and hypercalcemia. Destruction of bone
and its replacement by tumor may lead to pain, spinal cord
compression, and pathologic fracture.
.Bone pain: Bone pain is the most common presenting symptom in MM.
Most case series report that 70% of patients have bone pain at presentation.
The lumbar spine is one of the most common sites of pain.
.Spinal cord compression:The symptoms that should alert physicians to
consider spinal cord compression are back pain, weakness, numbness, or
dysesthesias in the extremities.
. Hypercalcemia:Confusion, somnolence, bone pain, constipation, nausea,
and thirst are the presenting symptoms of hypercalcemia.
8. 2.HEMATOLOGIC PROCESSES
Bone marrow infiltration by plasma cells results in neutropenia,
anemia, and thrombocytopenia. In terms of bleeding,a patient may
come to medical attention for bleeding resulting from
thrombocytopenia. Rarely, monoclonal protein may absorb clotting
factors and lead to bleeding.
.Anemia:Anemia, which may be quite severe, is the most common cause of
weakness in patients with MM.
.Hyperviscosity:This syndrome is infrequent in MM and occurs with IgG1,
IgG3, or IgA. MM may involve sludging in the capillaries, which results in
purpura, retinal hemorrhage, papilledema, coronary ischemia, or central
nervous system (CNS) symptoms (eg, confusion, vertigo, seizure).
.Cryoglobulinemia:causes Raynaud phenomenon, thrombosis, and
gangrene in the extremities.
9. 3. RENAL PROCESSES
The most common mechanisms of renal injury in MM are direct
tubular injury, amyloidosis, or involvement by plasmacytoma.Renal
conditions that may be observed include hypercalcemic nephropathy,
hyperuricemia due to renal infiltration of plasma cells resulting in
myeloma, light-chain nephropathy,amyloidosis,and
glomerulosclerosis.
10. 3. RENAL PROCESSES
Renal failure and insufficiency are seen in 25% of patients with
MM,including the following manifestations:
.Myeloma kidney syndrome with multiple etiologies
.Amyloidosis with light chains
.Nephrocalcinosis due to hypercalcemia
11. 4. NEUROLOGIC PROCESSES
The nervous system may be involved as a result of radiculopathy
and/or cord compression due to nerve compression and skeletal
destruction (amyloid infiltration of nerves).
Carpal tunnel syndrome is a common complication of myeloma.
Meningitis (especially that resulting from pneumococcal or
meningococcal infection) is more common in patients with MM. Some
peripheral neuropathies have been attributed to MM. Long-term
neurologic function is directly related to the rapidity of the diagnosis
and the institution of appropriate therapy for MM.
12. 5. INFECTION
Abnormal humoral immunity and leukopenia may lead to infection.
Pneumococcal organisms are commonly involved, but shingles (ie,
herpes zoster) and Haemophilus infections are also more common
among patients with MM.
13. PHYSICAL EXAMINATION
.On head, ears, eyes, nose, and throat (HEENT) examination, the eyes may
show exudative macular detachment, retinal hemorrhage, or cotton-wool
spots. Pallor from anemia may be present. Ecchymoses or purpura from
thrombocytopenia may be evident.
.Bony tenderness is not uncommon in MM.
.Neurologic findings may include a sensory level change.
.On evaluation of the abdomen, hepatosplenomegaly may be discovered.
.Amyloidosis may develop in some patients with MM. The characteristic
physical examination findings that suggest amyloidosis include the
following:
Shoulder pad sign
Macroglossia
Typical skin lesions
16. MGUS & SMM
Risk factors for progression to MM are as follows:
M protein concentration > 1.5 g/dL
Non-IgG isotype
An abnormal free light chain (FLC) ratio
Risk factors for progression of SMM to MM include any of the
following:
M protein concentration > 3 g/dL
Abnormal FLC ratio
Bone marrow plasma cell concentration > 10%
18. CHEMOTHERAPY
In patients with symptomatic MM, chemotherapy is required. In
asymptomatic patients with MM, treatment is delayed until disease
clinically progresses or until serum or urine levels of M protein
substantially increase.
The first step before starting therapy in MM is to determine whether a
patient is a candidate for an autologous stem cell transplant.
Eligibility depends primarily on the patient’s age and comorbidities.
Typically an age of 65 years is used as a cut-off point for transplant
eligibility.
Although a single drug may be used to treat multiple myeloma, more
often different kinds of drugs are used in combination. For example:
Melphalan and prednisone (MP), with or without thalidomide or
bortezomib. Vincristine, doxorubicin (Adriamycin), and
dexamethasone (called VAD)