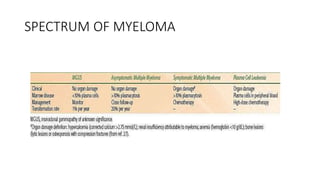
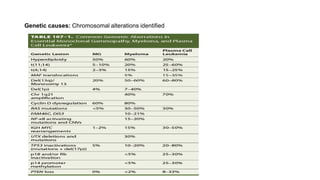
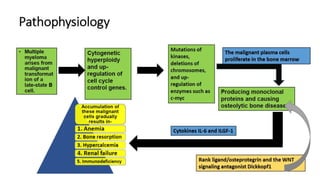
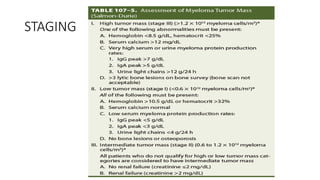
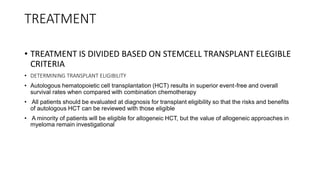
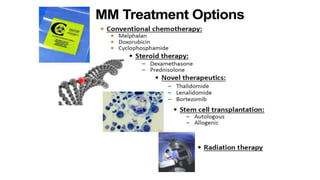
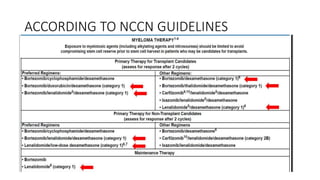
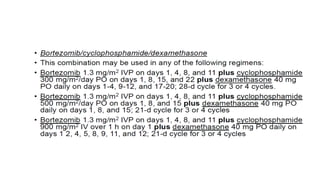
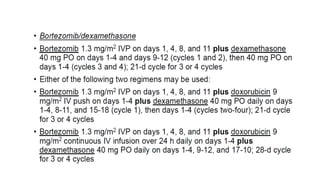
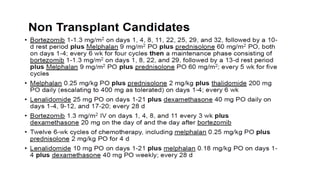
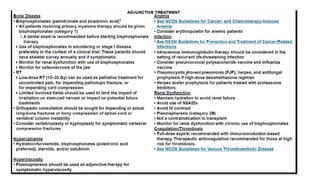
Multiple myeloma is a hematologic cancer caused by the clonal expansion of malignant plasma cells, leading to various complications such as anemia, bone disease, and renal dysfunction. The etiology is not completely understood, though factors include genetic alterations and environmental exposures. Diagnosis involves a comprehensive workup, and treatment options range from autologous stem cell transplantation to various chemotherapy regimens based on patient eligibility.