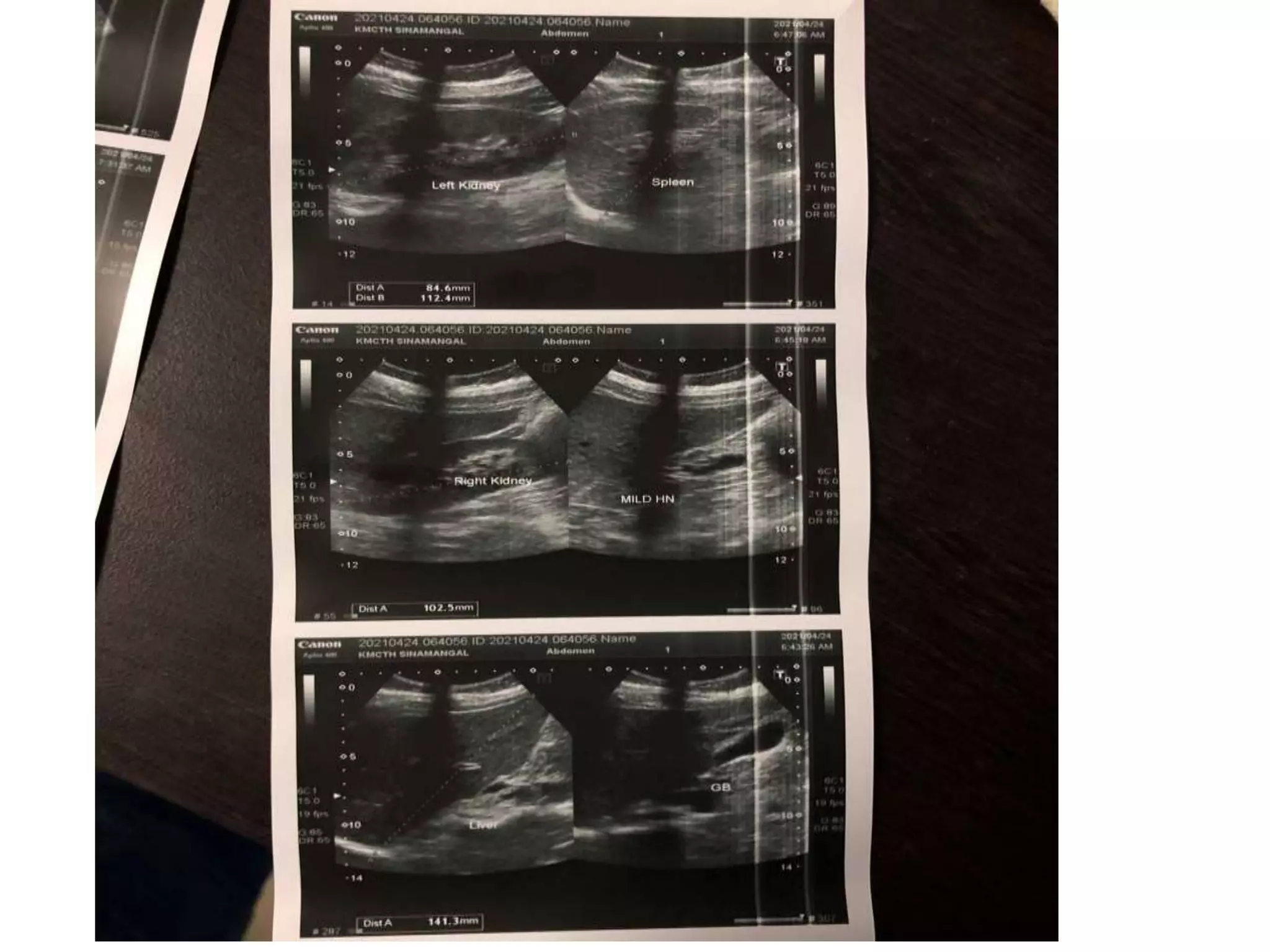
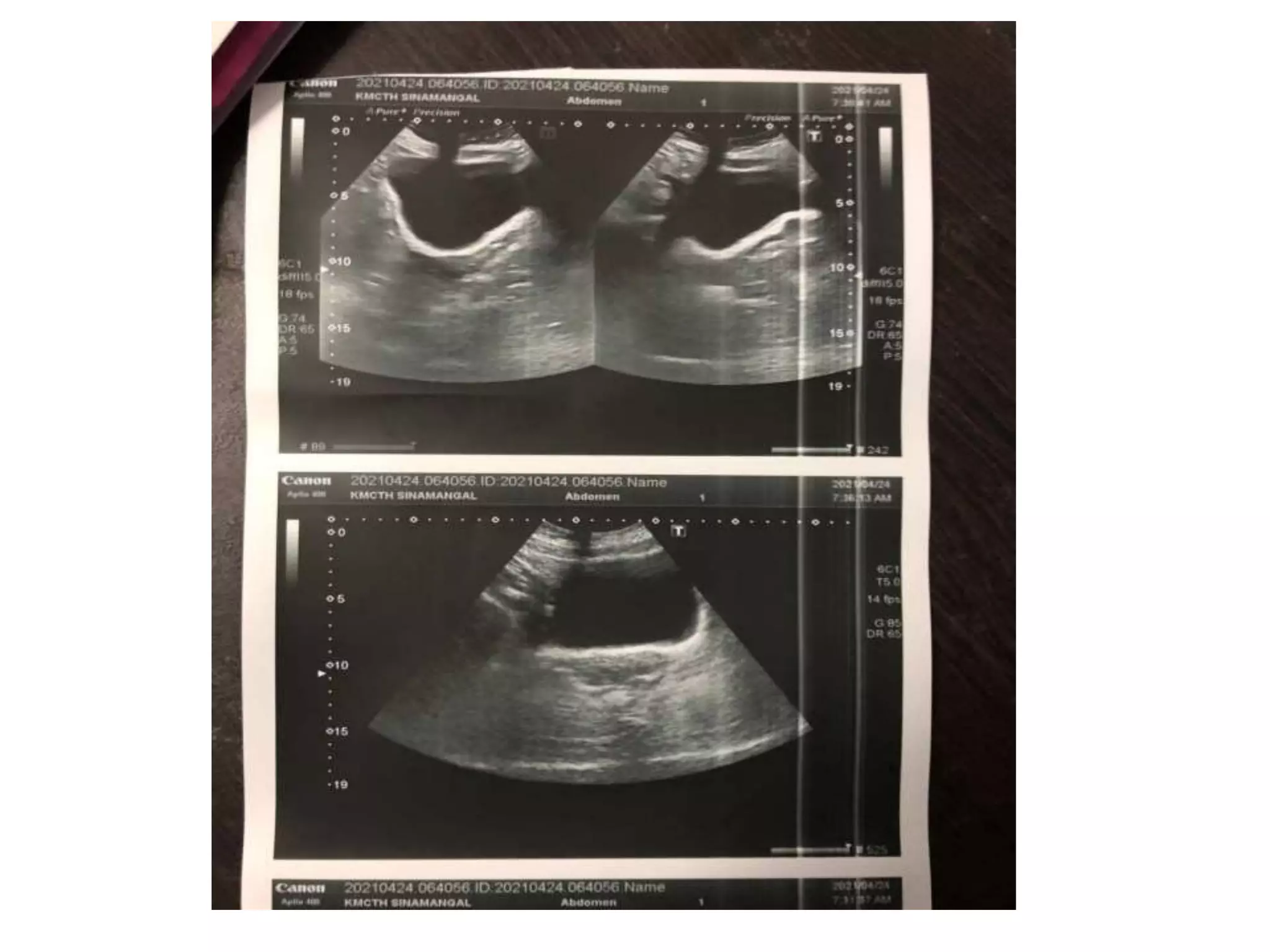
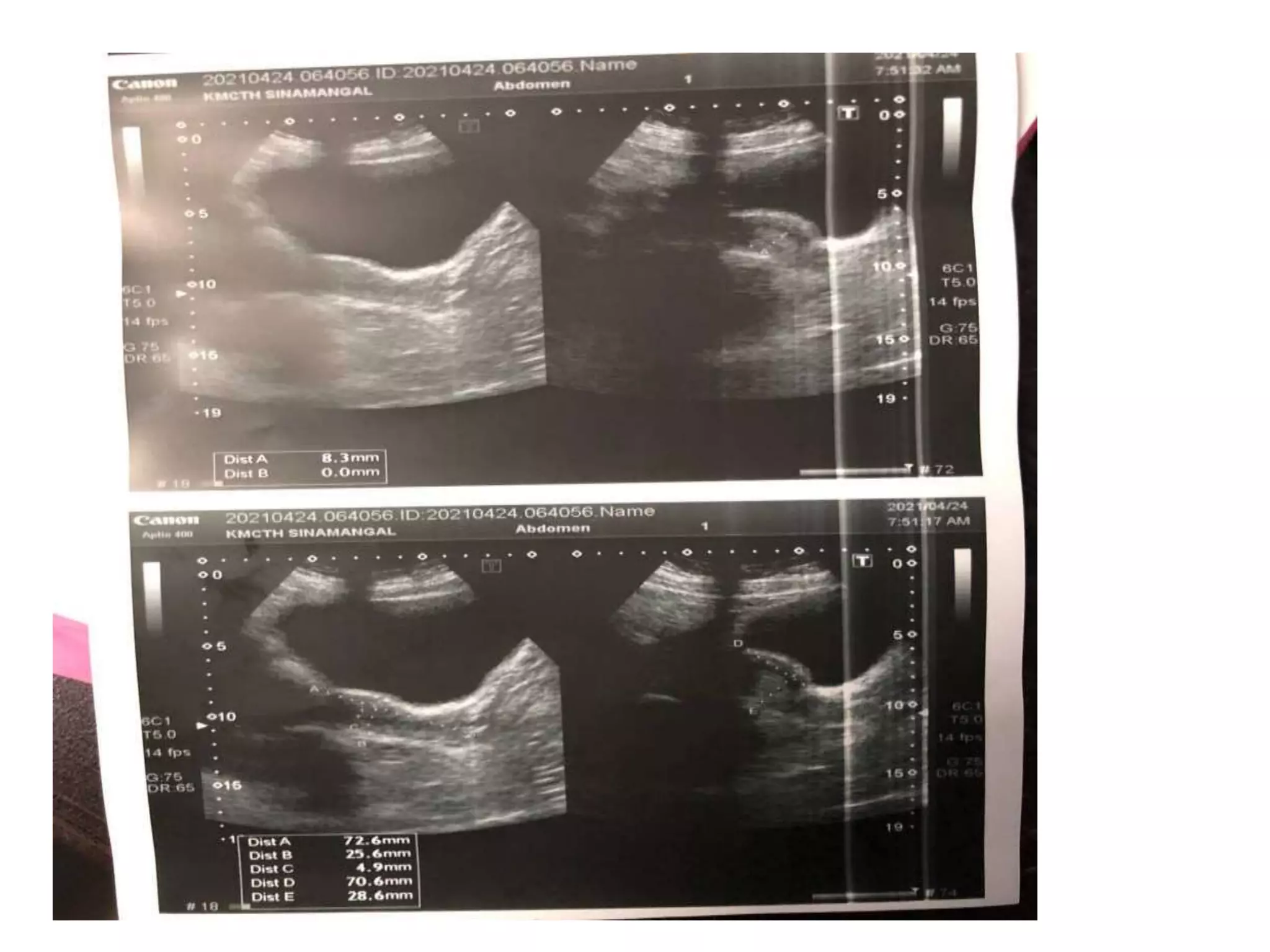
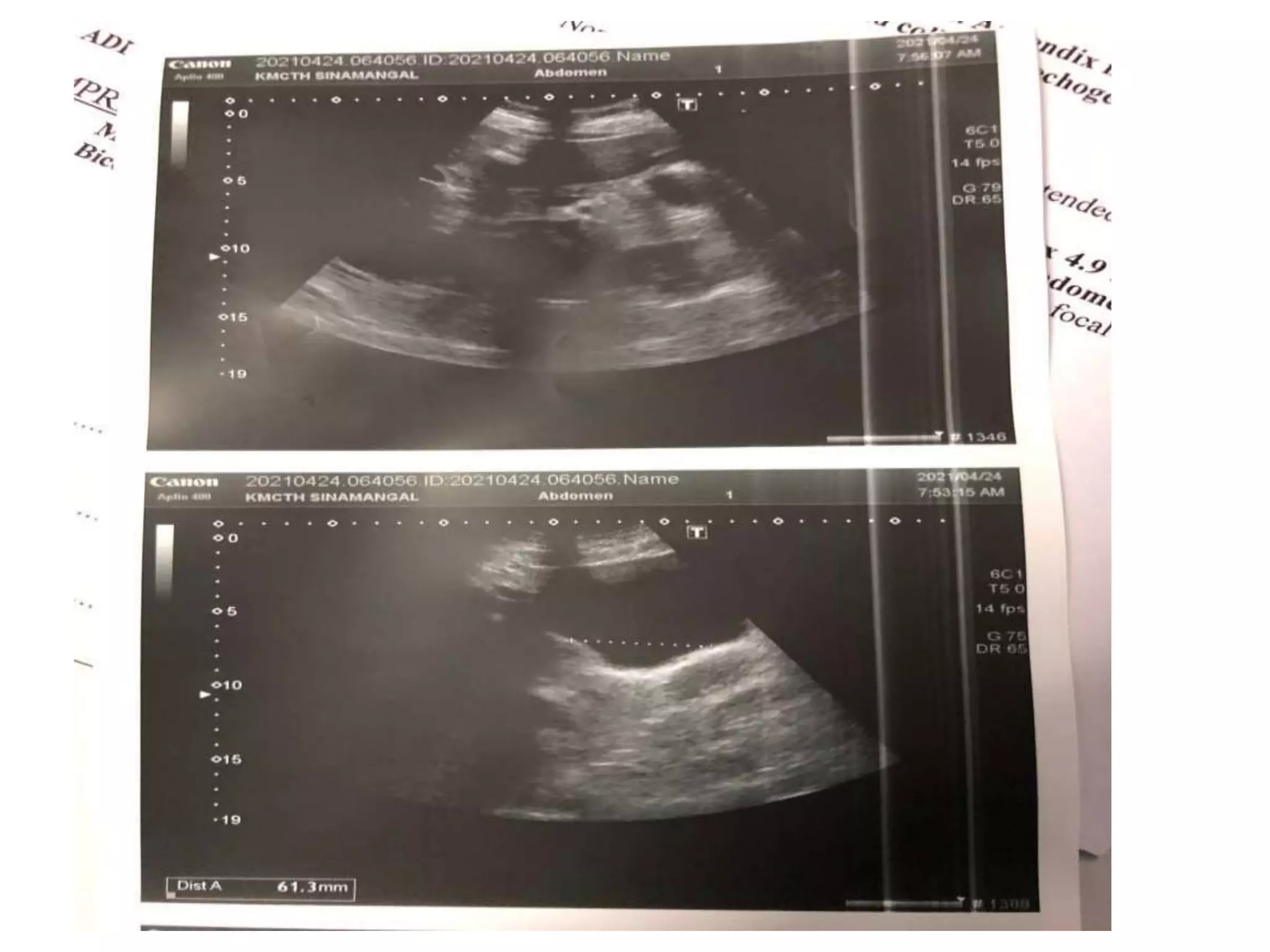
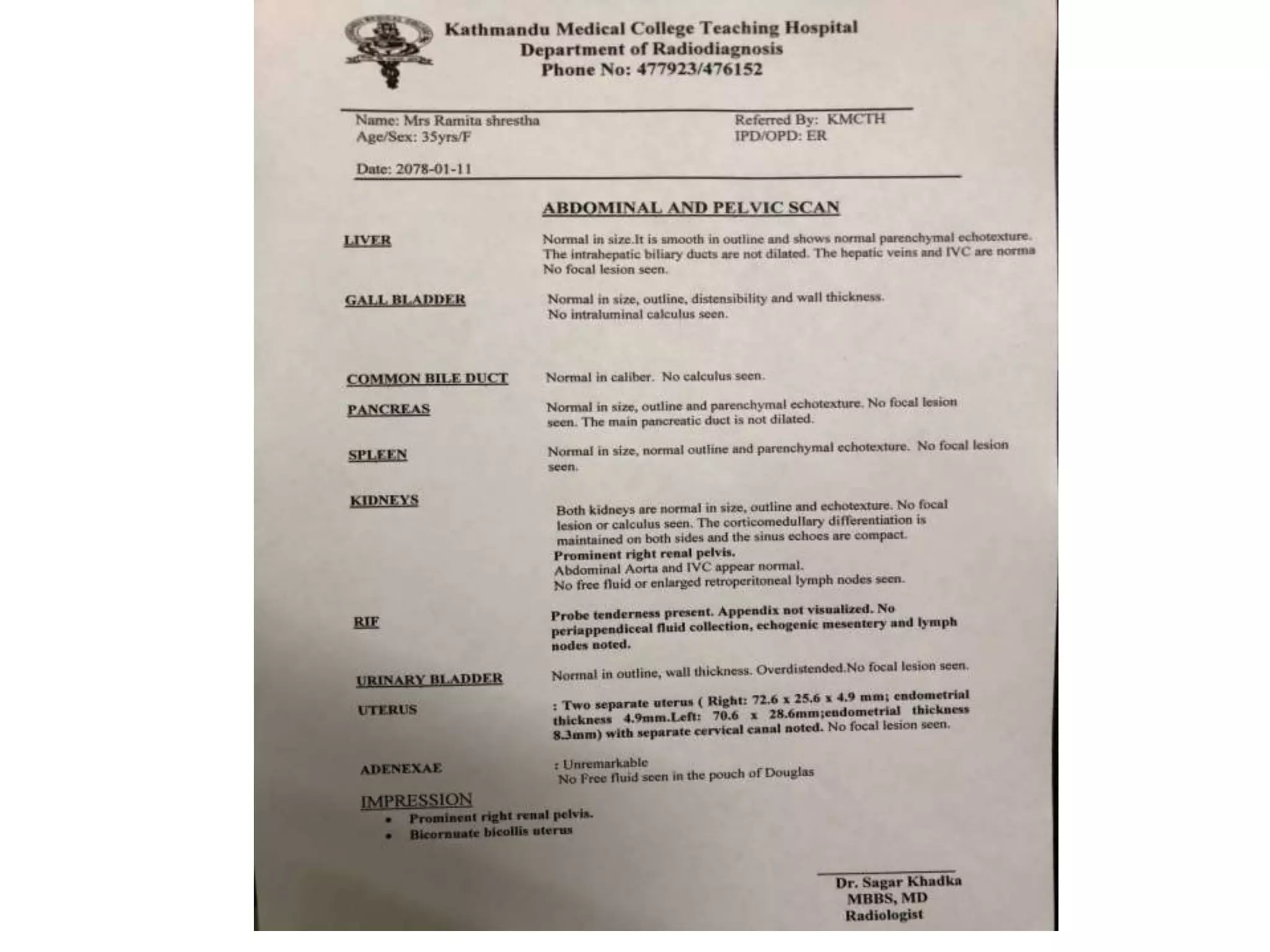
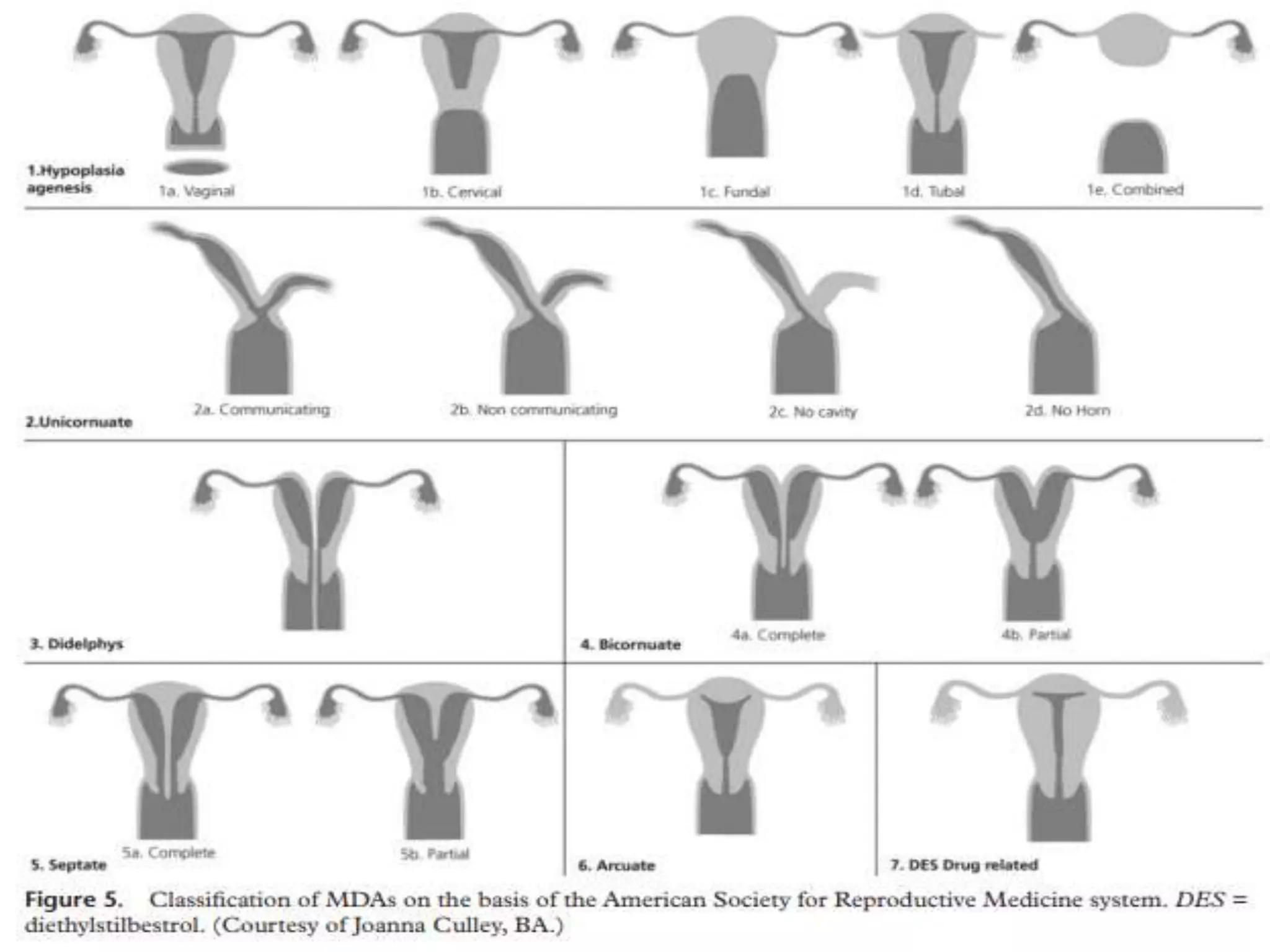
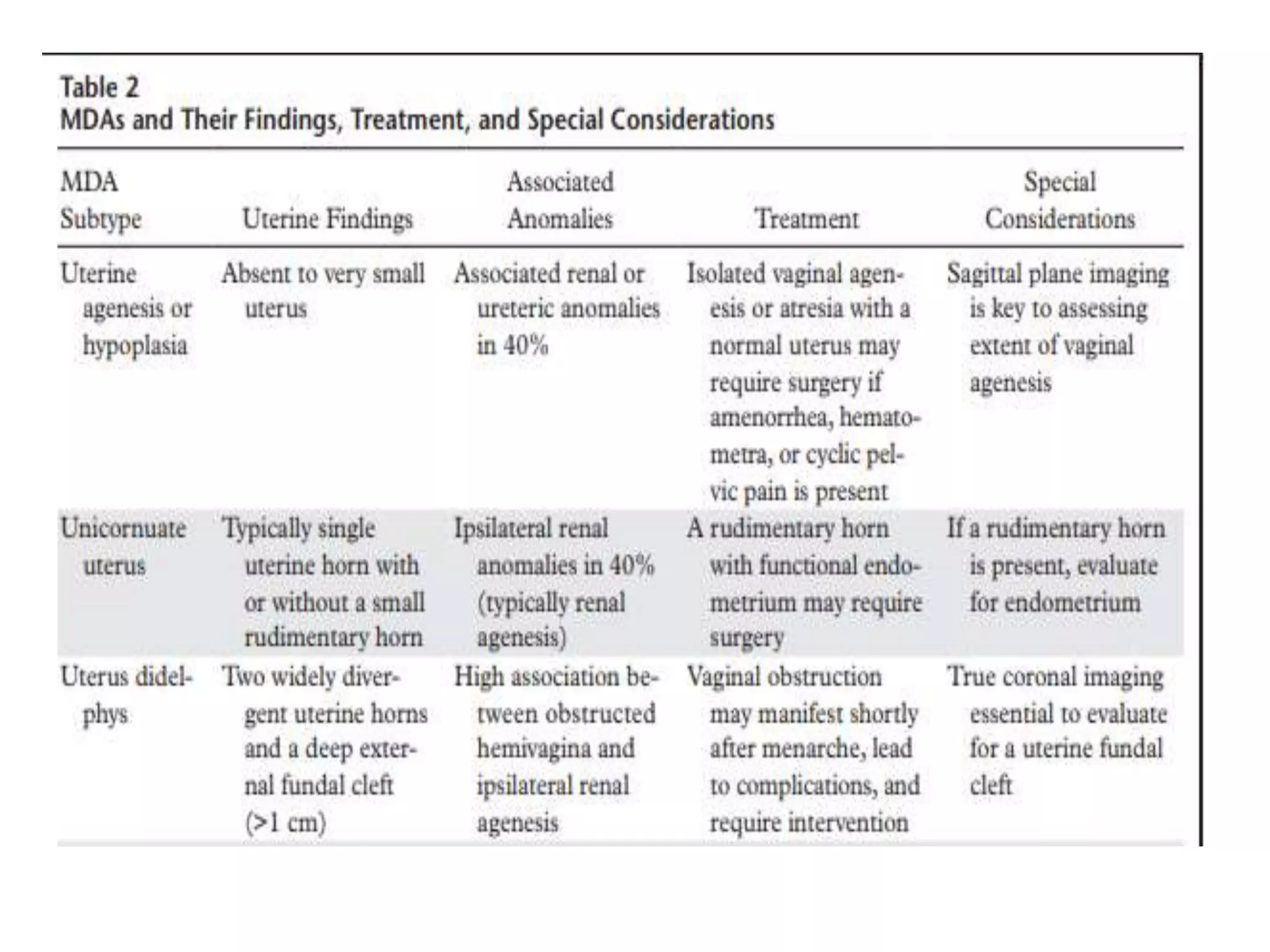
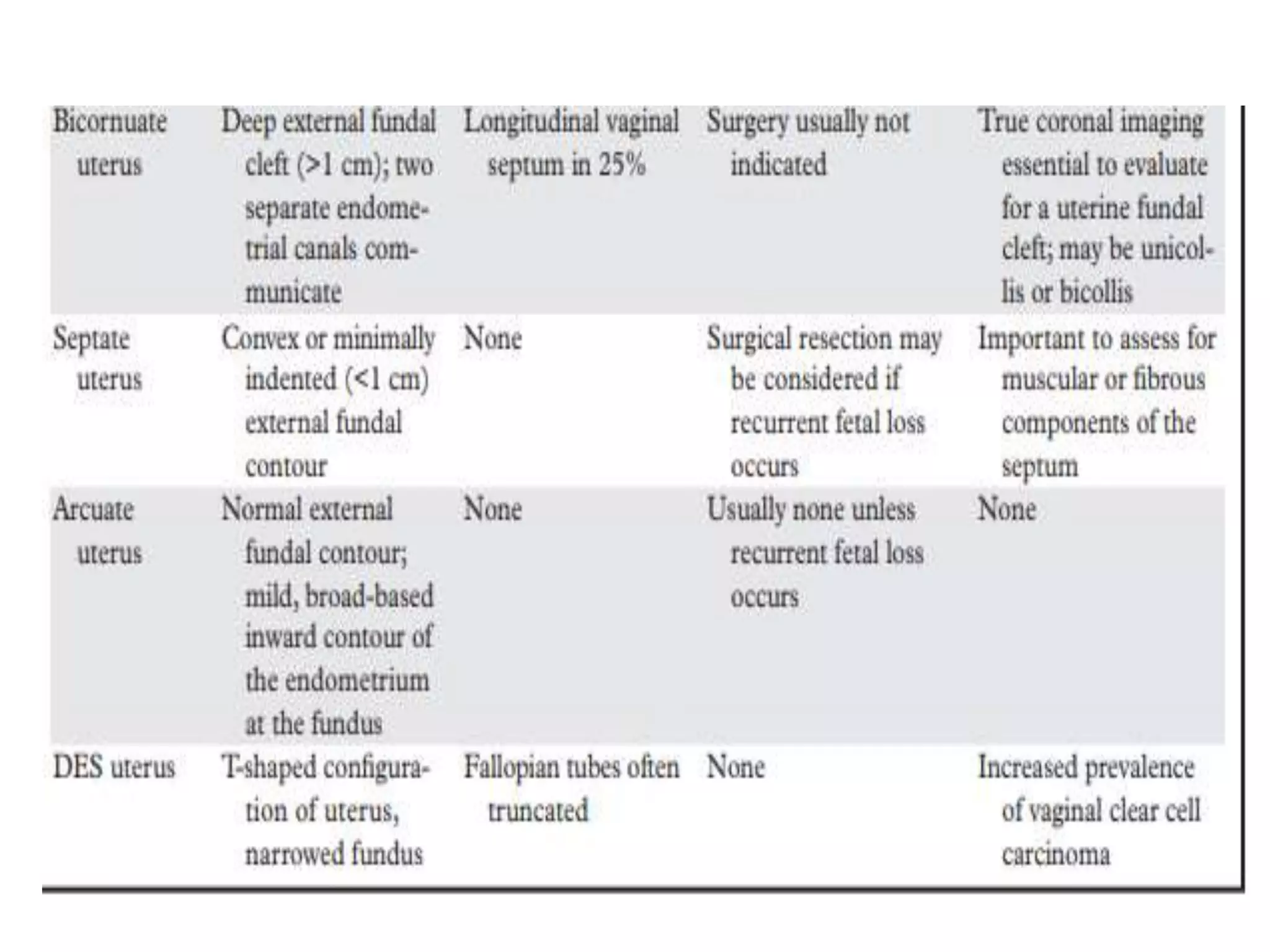
A 35-year-old woman presented with severe lower abdominal pain and difficulty urinating. An ultrasound revealed she had two separate uteruses with separate cervical canals but a normal vaginal canal, consistent with a bicornate bicollis uterus. This type of uterus is a müllerian duct anomaly that can result from interrupted development of the müllerian ducts in utero. Müllerian duct anomalies are associated with renal, vertebral, and cardiac anomalies as well as infertility and menstrual disturbances.