Downloaded 71 times
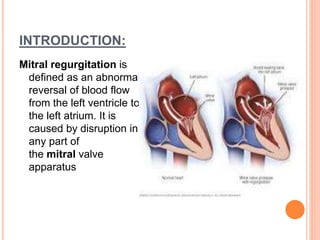
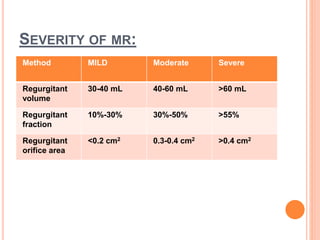
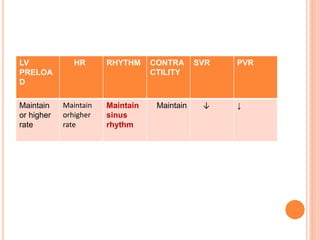


Mitral regurgitation occurs when blood flows backward from the left ventricle to the left atrium due to problems with the mitral valve. It can be caused by conditions like endocarditis or myocardial infarction. Hemodynamically, it decreases cardiac output and overloads the left atrium and lungs. Clinically, patients experience dyspnea, fatigue, edema and signs of pulmonary congestion. The severity is classified by the regurgitant volume and fraction. Treatment involves diuretics, vasodilators, and sometimes surgery. The anesthetic goals are to maintain forward flow by keeping heart rate and contractility normal while decreasing afterload and preload to limit regurgitant fraction. Induction and maintenance of







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










