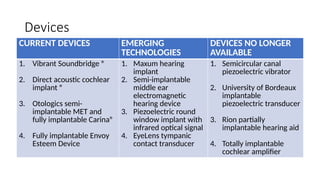
The document discusses middle ear implants, specifically the benefits and shortcomings of active middle ear implants (AMEI) compared to conventional hearing aids. It covers various types of AMEI, their designs, and mechanisms, as well as candidate selection criteria for these devices. Additionally, it highlights specific implant brands, their features, and considerations for patients with different types of hearing loss.