Downloaded 101 times

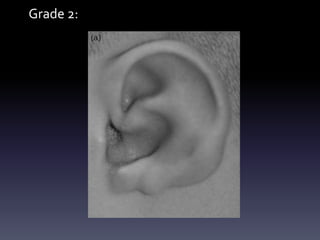
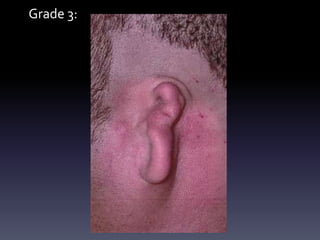
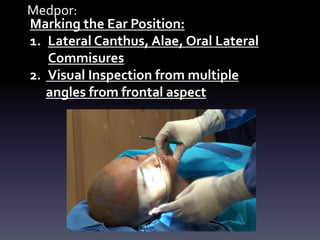


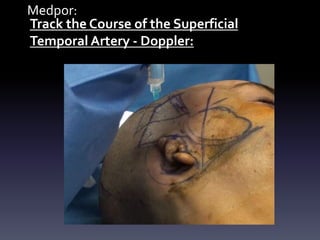

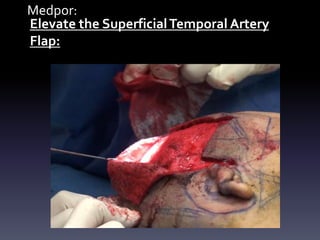









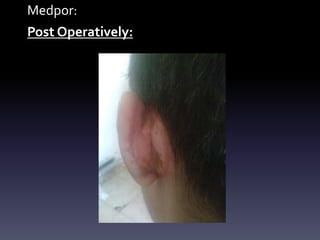
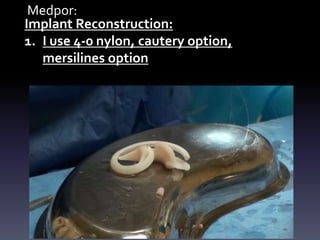
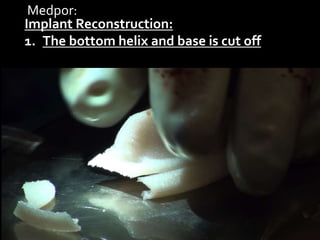

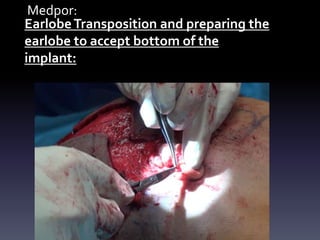



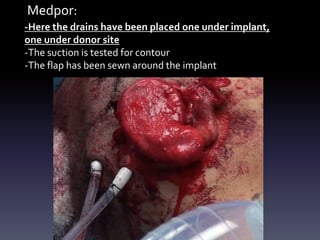




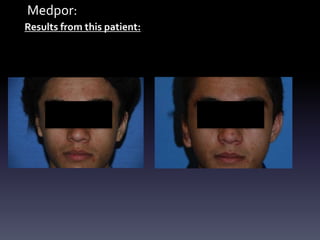


This document discusses microtia reconstruction using Medpor implants. It describes the grades of microtia from mild (Grade 1) to complete absence of the ear (Grade 4). The procedure involves marking positions, identifying arteries, elevating skin flaps, harvesting grafts, implant construction, placement and fixation, and closure. Key steps include harvesting contralateral and abdominal skin grafts, shaping the implant, securing the implant and transposing the earlobe. The results show initial swelling resolving over a month. Complications can include skin graft loss or exposure requiring further procedures.






























































![Untitled (6) [Autosaved] ear.pptx ear surgeries](https://cdn.slidesharecdn.com/ss_thumbnails/untitled6autosavedear-251128030434-d7ae6d96-thumbnail.jpg?width=640&height=640&fit=bounds)











