Downloaded 432 times
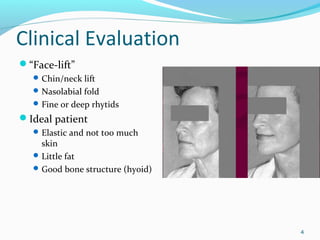
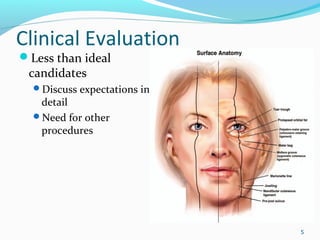
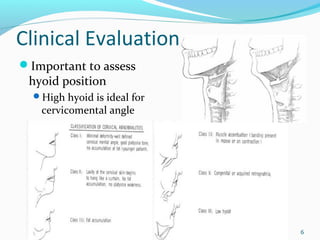
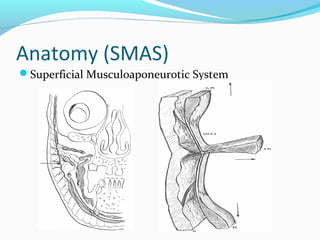
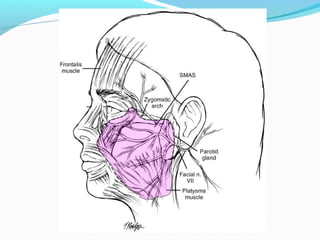
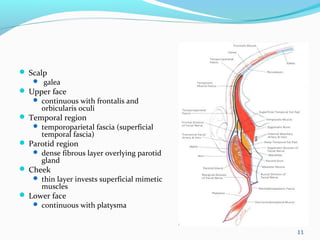
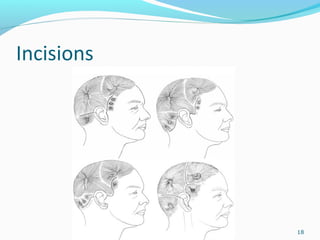
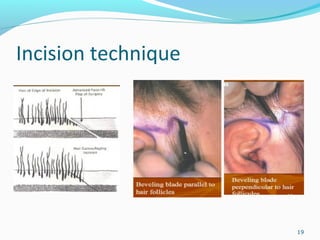
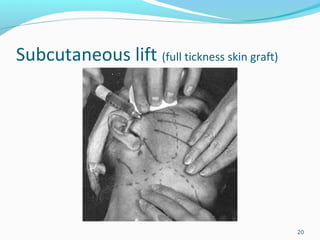
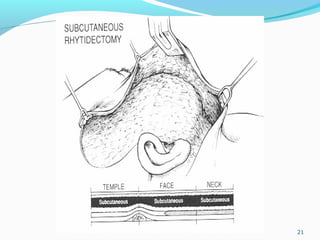
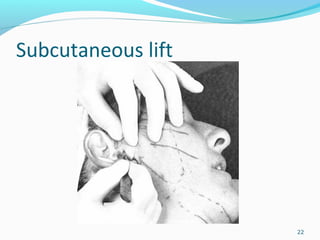
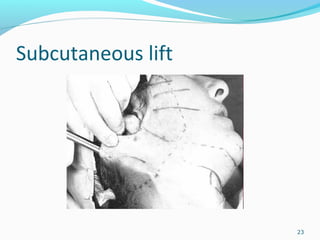
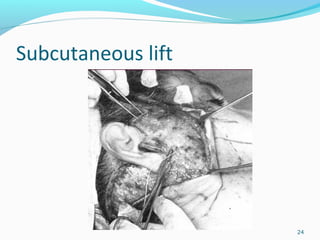
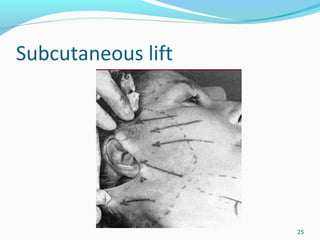
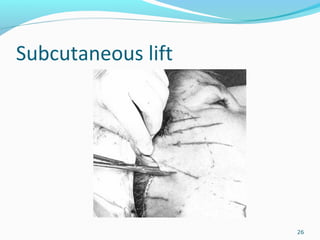
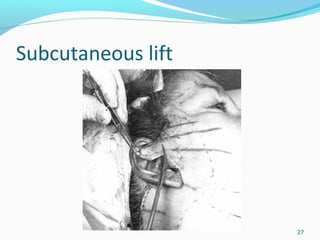
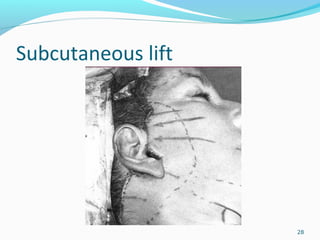
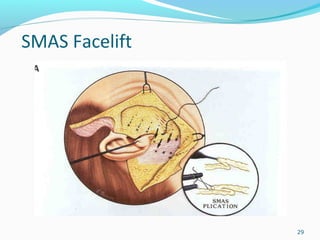
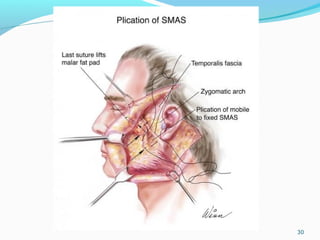
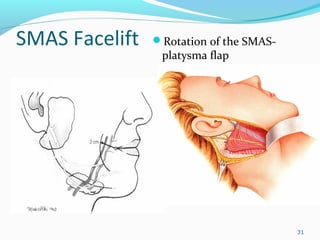
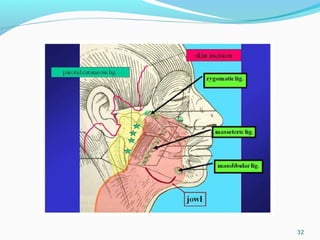
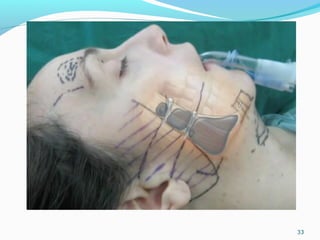
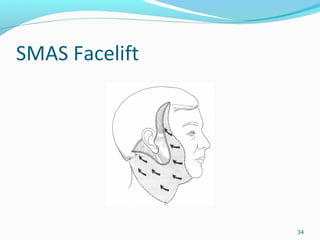


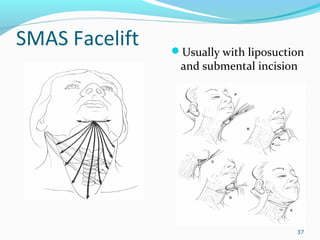
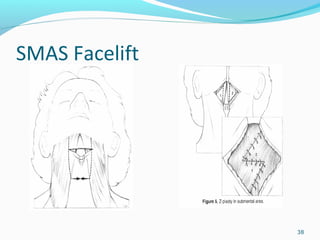
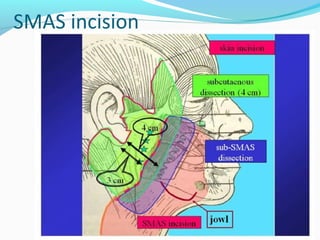
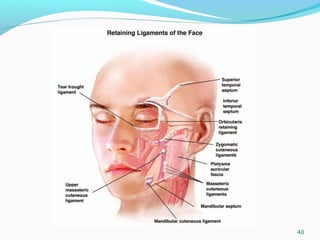
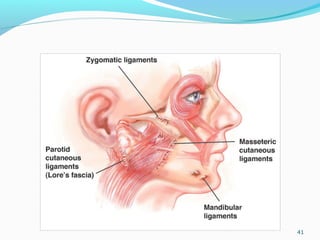
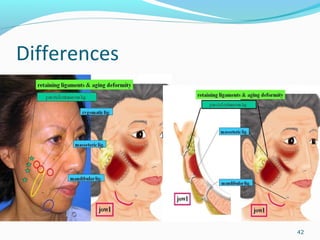
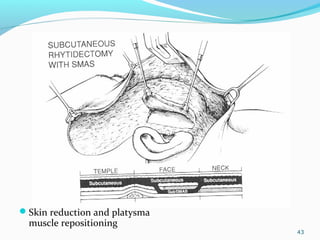
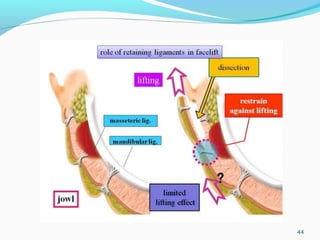
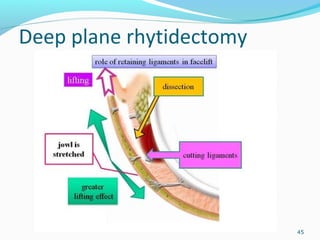
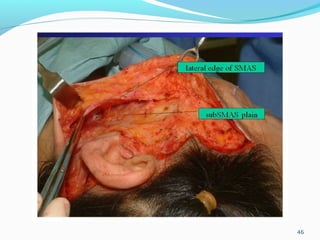

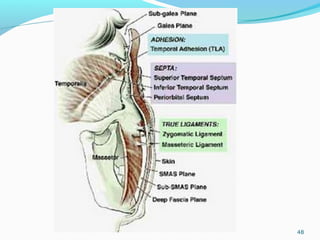
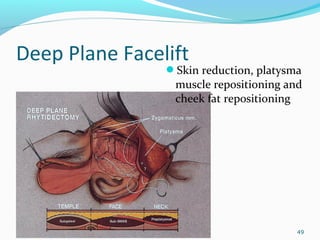
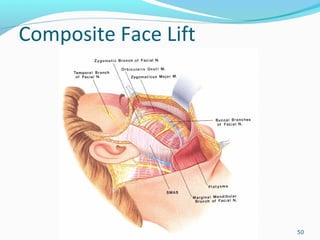
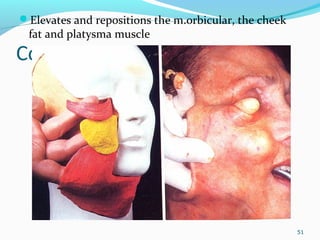
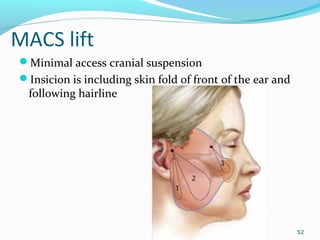

This document discusses preoperative evaluation and clinical evaluation for facelift surgery. It explores patient motivations and potential contraindications like diabetes or smoking. Ideal candidates are described as having elastic skin and good bone structure. The anatomy of the superficial musculoaponeurotic system (SMAS) is explained in detail. Various facelift techniques are outlined like subcutaneous lift, SMAS lift, and deep-plane lift. Incision sites, platysma muscle positioning, and suturing techniques are shown. Potential complications of facelift surgery are also listed.



































































