Downloaded 123 times


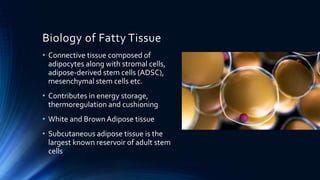


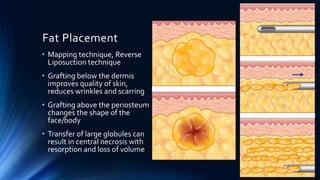




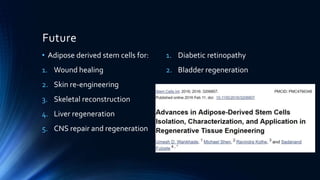


Fat grafting involves harvesting fat from areas like the abdomen through liposuction and refining it to separate viable fat cells from other components. The purified fat is then reinjected into areas like the face and breasts through microdroplet injections between skin layers to augment volume. Potential complications include irregular contours, necrosis of grafted fat, and infection. However, stem cells found in fat tissue are also being researched for uses like wound healing, skin engineering, and repairing various organs. Fat grafting is a popular aesthetic procedure that has been improved through techniques preserving high viability of transplanted fat cells.






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















