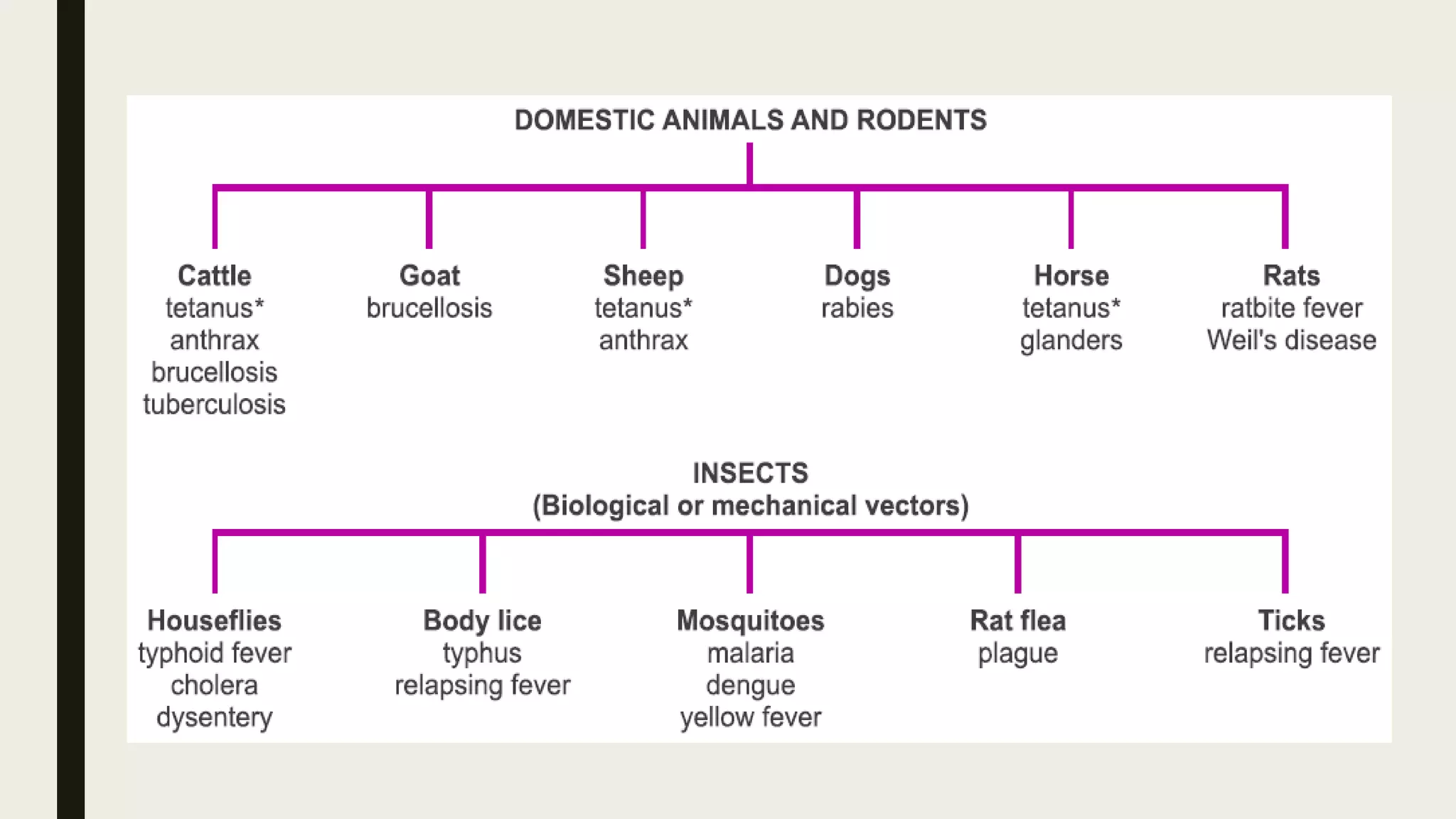
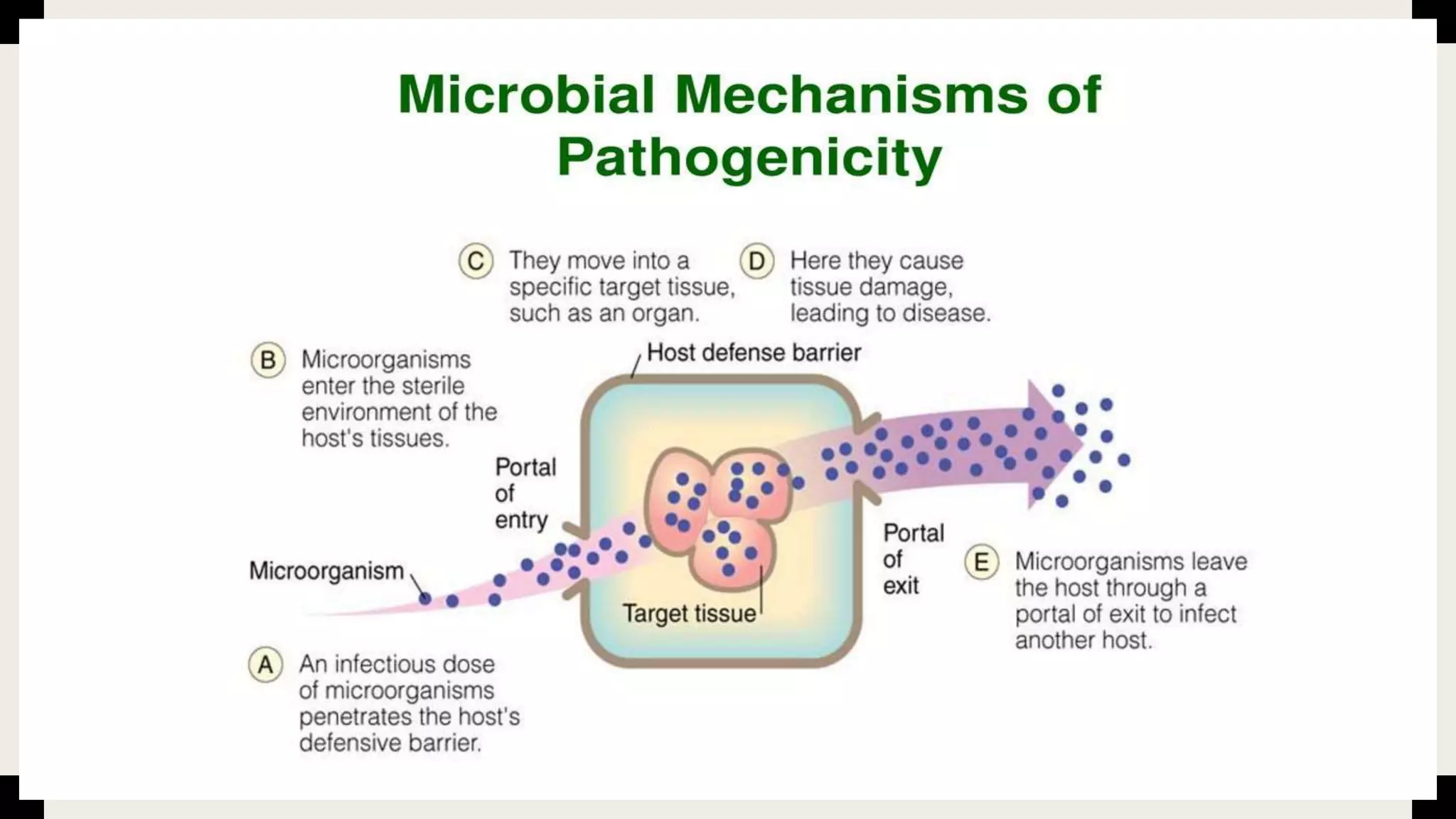
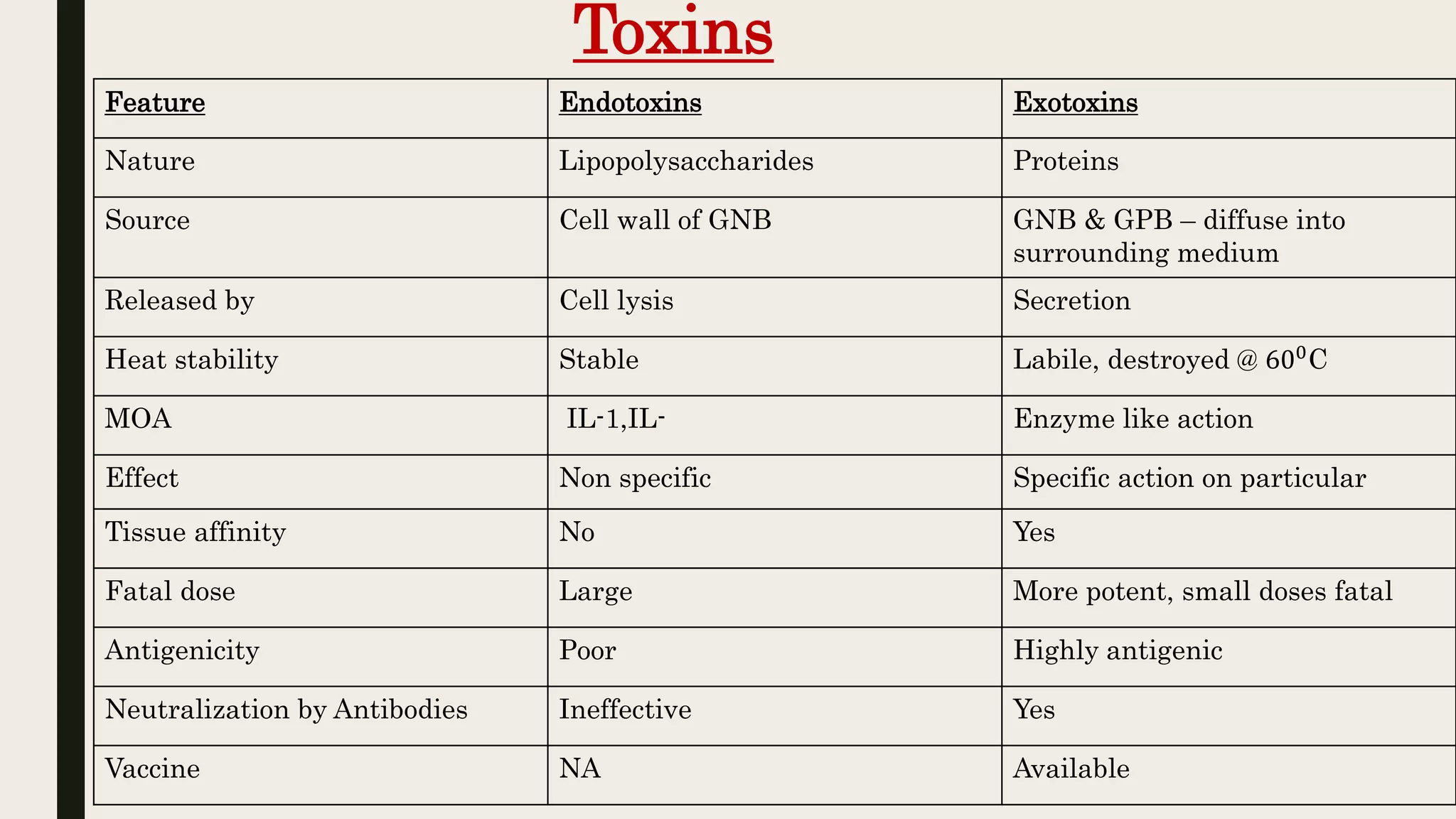
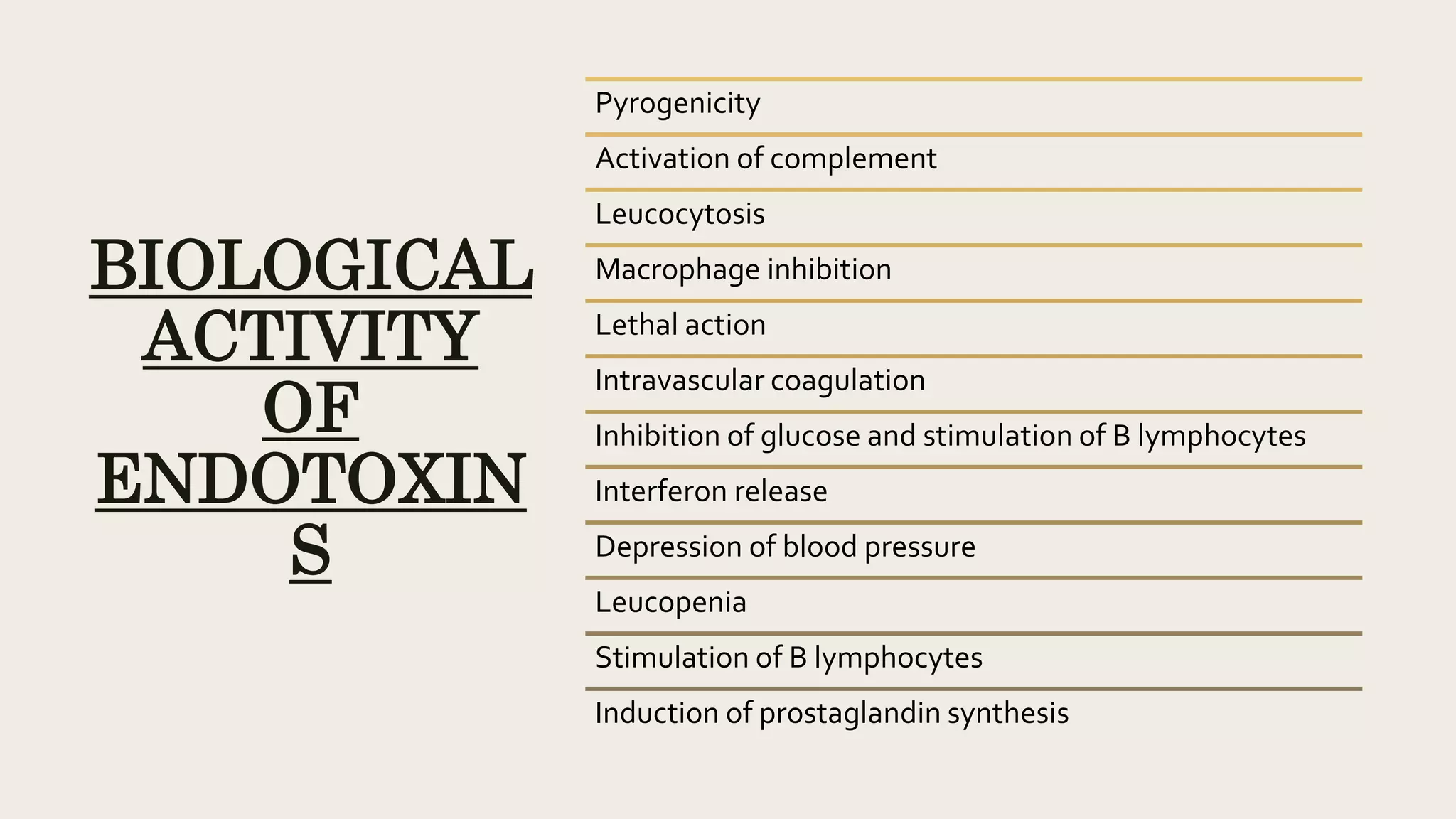
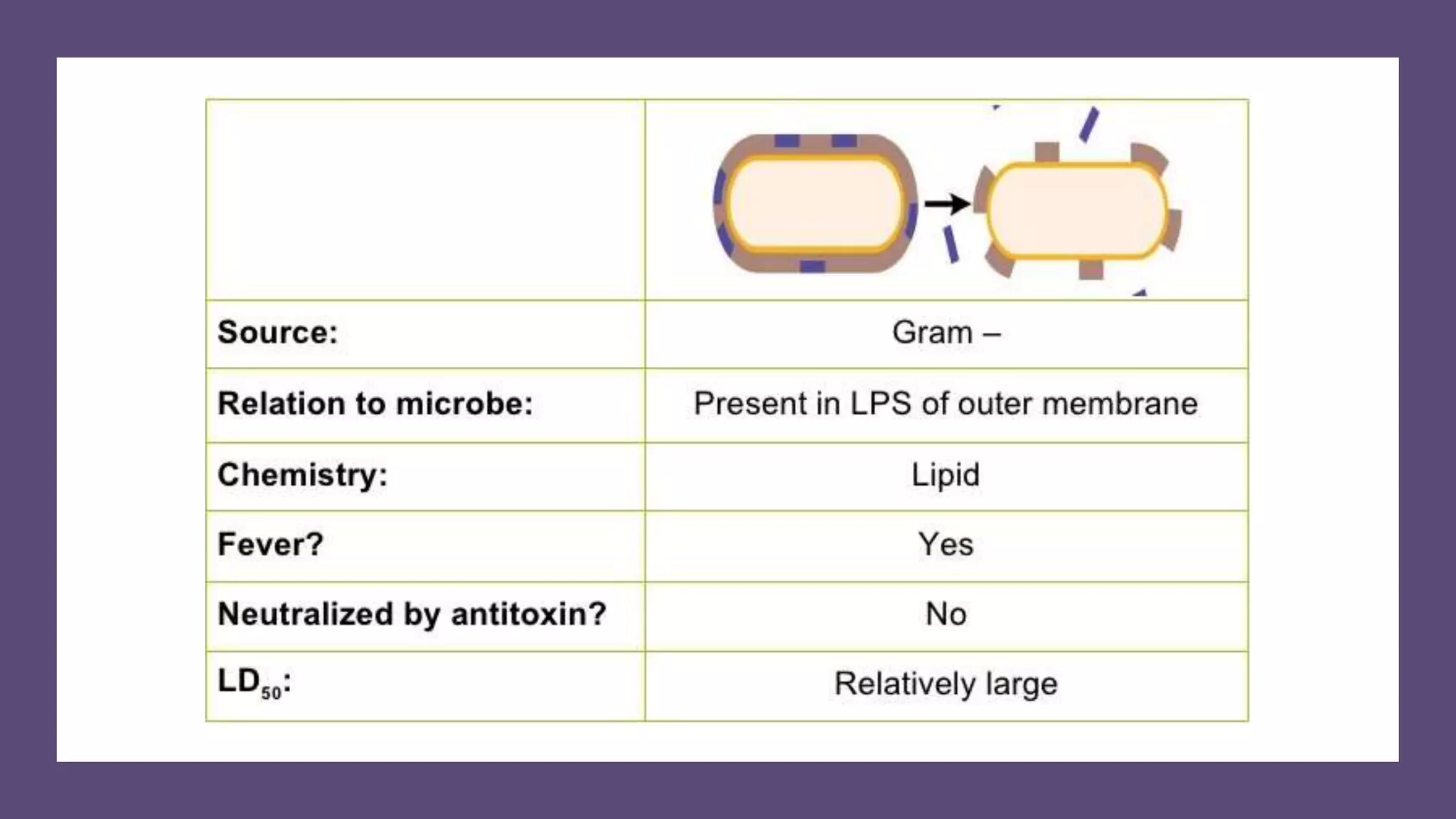
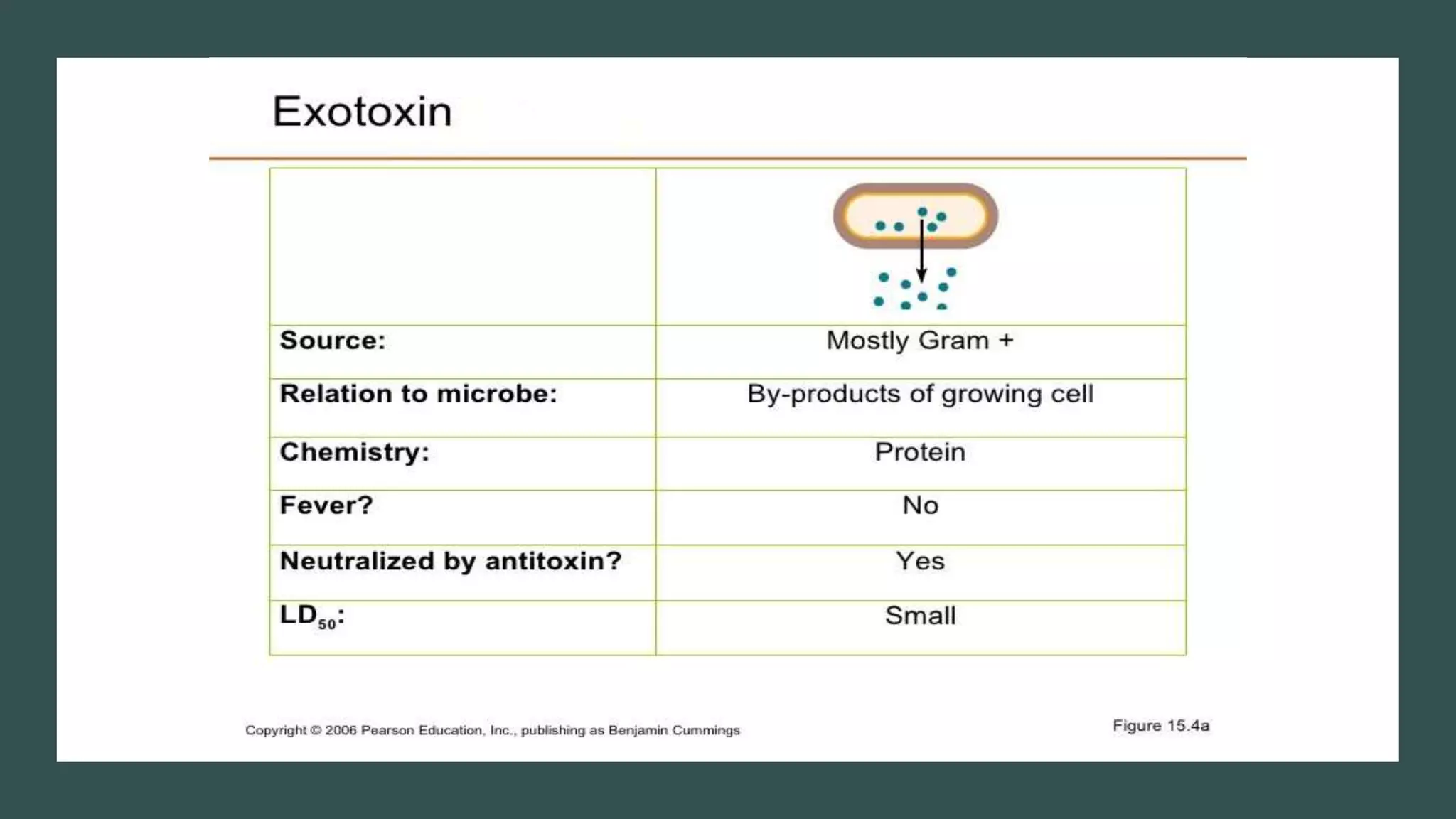
The document outlines various aspects of microbial pathogenicity, including classifications of pathogens (saprophytes, parasites, commensals, and opportunistic pathogens) and the processes of infection and disease. It describes different types of infectious diseases, their epidemiological patterns, and modes of transmission, as well as the mechanisms of microbial pathogenicity, including adhesion and virulence factors. The document also discusses the roles of reservoirs, carriers, and vectors in the spread of diseases, while highlighting the characteristics and effects of endotoxins and exotoxins.