Microbial Pathogenicity (classification and steps).pptx
To cause disease a pathogen must:
1. Gain access to the host
2. Adhere to host tissues
3. Penetrate or evade host defences
4. Damage the host, either:
- Directly
- Accumulation of microbial wastes
Animal & Microorganismsrelationship
• Saprophytes
– Free living microbes
– Dead & Decaying matter
– Except: B. subtilis (opportunistic infection)
• Parasites
– Microbes establish & multiply in host
– Pathogen: Produce disease
Commensals:
Live in harmony with host without causing disease
• Facultative pathogen: host resistance ↓ ↓
3.
DEFINITIONS
• Disease andInfectious Disease
– Disease
• Any deviation from a condition of good
health and well-being
– Infectious Disease
· A disease condition caused by the presence
or growth of infectious microorganisms or
parasites
4.
Entry of pathogen:
•Infection:
– Pathogen enter----establish ---invade Normal anatomical barrier---multiply—
infection
– Lodgement & multiplication of pathogen in or on tissue of host
– Infection-disease
• Colonization
– Pathogen enter—multiply—not invade/elicit immune response
5.
Classification of Infections
•Acute infection vs. chronic infection
– Acute Infection
• An infection characterized by sudden onset,
rapid progression, and often with severe
symptoms
– Chronic Infection
• An infection characterized by delayed onset
and slow progression
6.
• Primary infectionvs. secondary infection
– Primary Infection
• An infection that develops in an otherwise healthy
individual
– Secondary Infection
• An infection that develops in an individual who is already
infected with a different pathogen
7.
• Localized infectionvs. systemic infection
– Localized Infection
• An infection that is restricted to a specific location or
region within the body of the host
– Systemic Infection
• An infection that has spread to several regions or areas in
the body of the host
8.
• Clinical, subclinical,atypical, Latent infection
– Clinical Infection
• An infection with obvious observable or detectable symptoms
– Subclinical/ Asymptomatic Infection
• An infection with few or no obvious symptoms with active infection
– Atypical Infection
• No characteristic
– Latent infection
• Infection—inactive or dormant latent/hidden form—↓↓ host resistance---
proliferation of pathogen---Disease
9.
• Opportunistic infection
–An infection caused by microorganisms that are
commonly found in the host’s environment.
This term is often used to refer to infections
caused by organisms in the normal flora
10.
DEFINITIONS
• The suffix“-emia”
– A suffix meaning “presence of an infectious agent”
• Bacteremia = Presence of infectious bacteria
• Viremia = Presence of infectious virus
• Fungemia = Presence of infectious fungus
• Septicemia = Presence of an infectious agent in
the bloodstream
11.
Source ….Reservoir
Source:
Person/Animal/Object from which a microorganism is
transmitted to host
Reservoir:
Natural habitat in which organism multiply, live.
Maintain parasite in nature
Asymptomatic infection
CARRIERS
• Carriers
– Person/infectious agent in absence of clinical symptom & Shed from
body via contact, air or secretions
– Inadequate Treatment/Immune response ---incomplete elimination of
organism
– Less infectious than Cases BUT More Dangerous
• Types:
– Incubatory carrier: These people can spread a pathogen before they
show symptoms of the illness.
Eg. Measels, Mumps, Polio, Hepatitis B, Influenza, Diphtheria
etc
– Healthy carrier: Subclinical infection without suffering from disease
converted into carrier eg. Diphtheria etc.
– Convalescent carrier: Recovered from disease but still continue to
harbour pathogen-shed from body
14.
CARRIERS
• Based onduration:
– Temporary carrier: <6months duration
Healthy, incubatory, convalescent carrier
– Chronic carrier: Indefinite period
Hepatitis B, Typhoid
• Based on Source:
– Contact carrier: acquire pathogen from patient
– Paradoxical carrier: Acquire infection from another carrier
15.
MODE OF TRANSMISSION
•Contact
– Direct: STD
– Indirect: by objects
• Inhalational
process of breathing in
• Ingestion
• Inoculation/ Percutaneous
– Animal bite
– Direct inoculation into tissue following injury
– blood borne infections
MODE OF TRANSMISSION
•Vertical
– Transplacental: TORCH
– ( toxoplasmosis, others(Syphilis, Hepatitis B), rubella, Cytomegalovirus
(CMV by HHV-5), and herpes simplex virus )
– During passage through birth canal: Gp B streptococcus,
HIV
• Laboratory induced
18.
MICROBIAL PATHOGENICITY
o Pathogenicity= ability to cause disease
o Virulence = degree of pathogenicity
o Pathogens must first gain access to the host
o Must adhere and penetrate before infection is
established
o Then must continually evade host defenses
o Infection usually causes host damage: disease
19.
VIRULENCE VARIATIONS
o SPONTANEOUS
oINDUCED
↓----ATTENUATION
o Passage in unfavourable conditions
o Repeated subculture artificial media
o Prolonged storage
o Growth in presence of inhibitors/high temperature
↑---EXALTATION
o Serial passage in susceptible host
20.
MICROBIAL PATHOGENICITY
o Tocause disease a pathogen must:
o 1. Gain access to the host
o 2. Adhere to host tissues
o 3. Penetrate or evade host defences
o 4. Damage the host, either:
- Directly
- Accumulation of microbial wastes
ENTRY INTO HOST
1.Portals of Entry
A. Mucus membranes (moist mucosa)
-most common route for most pathogens
-entry through mucus membranes:
1. respiratory tract (most common)
2. gastrointestinal tract
3. urinary/genital tracts
4. conjunctiva
23.
ENTRY INTO HOST
B.Skin (keratinized cutaneous membrane)
-some pathogens infect hair follicles and
sweat glands
-few can colonize surface
-unless broken, skin is usually an
impermeable barrier to microbes
24.
ENTRY INTO HOST
C.Penetral route
• penetrate skin: punctures,
injections, bites, cuts, surgery, etc.
• deposit organisms directly into
deeper tissues
• most microbes must enter through
their preferred portal of entry in
order to cause disease
• some can cause disease from many
routes of entry
• most usually also exit the host from
the same original portal to spread
disease
25.
ENTRY INTO HOST
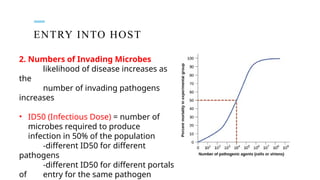
2.Numbers of Invading Microbes
likelihood of disease increases as
the
number of invading pathogens
increases
• ID50 (Infectious Dose) = number of
microbes required to produce
infection in 50% of the population
-different ID50 for different
pathogens
-different ID50 for different portals
of entry for the same pathogen
26.
ENTRY INTO HOST
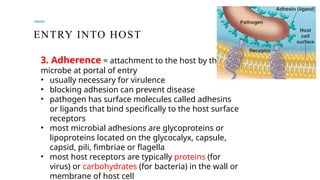
3.Adherence = attachment to the host by the
microbe at portal of entry
• usually necessary for virulence
• blocking adhesion can prevent disease
• pathogen has surface molecules called adhesins
or ligands that bind specifically to the host surface
receptors
• most microbial adhesions are glycoproteins or
lipoproteins located on the glycocalyx, capsule,
capsid, pili, fimbriae or flagella
• most host receptors are typically proteins (for
virus) or carbohydrates (for bacteria) in the wall or
membrane of host cell
27.
ENTRY INTO HOST
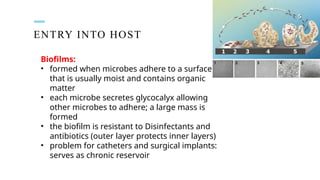
Biofilms:
•formed when microbes adhere to a surface
that is usually moist and contains organic
matter
• each microbe secretes glycocalyx allowing
other microbes to adhere; a large mass is
formed
• the biofilm is resistant to Disinfectants and
antibiotics (outer layer protects inner layers)
• problem for catheters and surgical implants:
serves as chronic reservoir
28.
PENETRATION OF HOSTDEFENCES
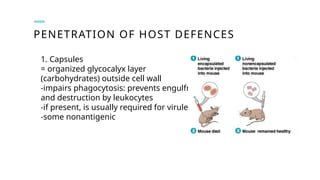
1. Capsules
= organized glycocalyx layer
(carbohydrates) outside cell wall
-impairs phagocytosis: prevents engulfment
and destruction by leukocytes
-if present, is usually required for virulence
-some nonantigenic
29.
PENETRATION OF HOSTDEFENCES
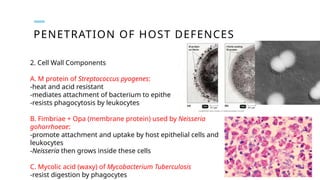
2. Cell Wall Components
A. M protein of Streptococcus pyogenes:
-heat and acid resistant
-mediates attachment of bacterium to epithelial cells
-resists phagocytosis by leukocytes
B. Fimbriae + Opa (membrane protein) used by Neisseria
gohorrhoeae:
-promote attachment and uptake by host epithelial cells and
leukocytes
-Neisseria then grows inside these cells
C. Mycolic acid (waxy) of Mycobacterium Tuberculosis
-resist digestion by phagocytes
30.
PENETRATION OF HOSTDEFENCES
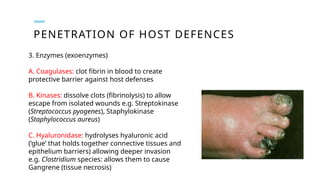
3. Enzymes (exoenzymes)
A. Coagulases: clot fibrin in blood to create
protective barrier against host defenses
B. Kinases: dissolve clots (fibrinolysis) to allow
escape from isolated wounds e.g. Streptokinase
(Streptococcus pyogenes), Staphylokinase
(Staphylococcus aureus)
C. Hyaluronidase: hydrolyses hyaluronic acid
(‘glue’ that holds together connective tissues and
epithelium barriers) allowing deeper invasion
e.g. Clostridium species: allows them to cause
Gangrene (tissue necrosis)
31.
PENETRATION OF HOSTDEFENCES
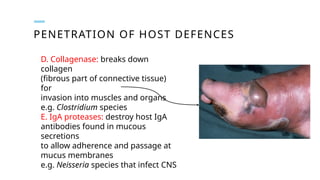
D. Collagenase: breaks down
collagen
(fibrous part of connective tissue)
for
invasion into muscles and organs
e.g. Clostridium species
E. IgA proteases: destroy host IgA
antibodies found in mucous
secretions
to allow adherence and passage at
mucus membranes
e.g. Neisseria species that infect CNS
32.
PENETRATION OF HOSTDEFENCES
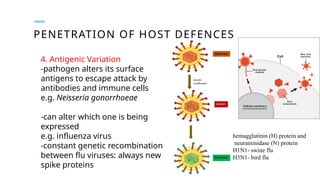
4. Antigenic Variation
-pathogen alters its surface
antigens to escape attack by
antibodies and immune cells
e.g. Neisseria gonorrhoeae
-can alter which one is being
expressed
e.g. influenza virus
-constant genetic recombination
between flu viruses: always new
spike proteins
hemagglutinin (H) protein and
neuraminidase (N) protein
H1N1- swine flu
H5N1- bird flu
33.
PENETRATION OF HOSTDEFENCES
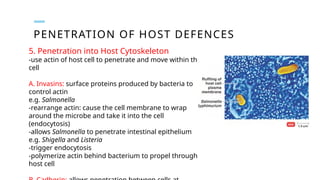
5. Penetration into Host Cytoskeleton
-use actin of host cell to penetrate and move within the
cell
A. Invasins: surface proteins produced by bacteria to
control actin
e.g. Salmonella
-rearrange actin: cause the cell membrane to wrap
around the microbe and take it into the cell
(endocytosis)
-allows Salmonella to penetrate intestinal epithelium
e.g. Shigella and Listeria
-trigger endocytosis
-polymerize actin behind bacterium to propel through
host cell
34.
DAMAGE TO HOSTCELLS
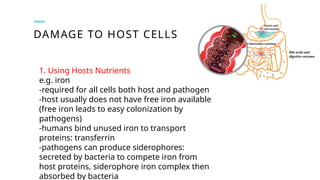
1. Using Hosts Nutrients
e.g. iron
-required for all cells both host and pathogen
-host usually does not have free iron available
(free iron leads to easy colonization by
pathogens)
-humans bind unused iron to transport
proteins: transferrin
-pathogens can produce siderophores:
secreted by bacteria to compete iron from
host proteins, siderophore iron complex then
absorbed by bacteria
35.
DAMAGE TO HOSTCELLS
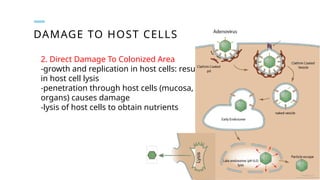
2. Direct Damage To Colonized Area
-growth and replication in host cells: results
in host cell lysis
-penetration through host cells (mucosa,
organs) causes damage
-lysis of host cells to obtain nutrients
36.
DAMAGE TO HOSTCELLS
3. Production of Toxins
Toxins = poisonous substance produced by microbes
-tend to cause widespread damage/disease in host
-may be necessary for virulence
A. Exotoxins
-produced inside the bacteria and either secreted or released following microbe
lysis
-toxin genes are often found on plasmids or via lysogenic phages
-most are enzymes
-function to destroy certain host cell parts or inhibit particular metabolic
functions
-damage from toxin results in the particular signs or symptoms of a disease
-can be named for the disease, type of cell attacked or organism that produces it
e.g. tetanus toxin: causes tetanus (contraction) of muscle
37.
DAMAGE TO HOSTCELLS
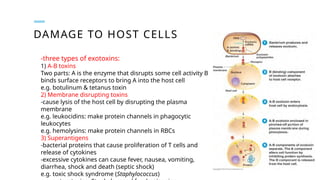
-three types of exotoxins:
1) A-B toxins
Two parts: A is the enzyme that disrupts some cell activity B
binds surface receptors to bring A into the host cell
e.g. botulinum & tetanus toxin
2) Membrane disrupting toxins
-cause lysis of the host cell by disrupting the plasma
membrane
e.g. leukocidins: make protein channels in phagocytic
leukocytes
e.g. hemolysins: make protein channels in RBCs
3) Superantigens
-bacterial proteins that cause proliferation of T cells and
release of cytokines
-excessive cytokines can cause fever, nausea, vomiting,
diarrhea, shock and death (septic shock)
e.g. toxic shock syndrome (Staphylococcus)
38.
DAMAGE TO HOSTCELLS
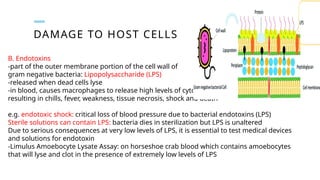
B. Endotoxins
-part of the outer membrane portion of the cell wall of
gram negative bacteria: Lipopolysaccharide (LPS)
-released when dead cells lyse
-in blood, causes macrophages to release high levels of cytokines
resulting in chills, fever, weakness, tissue necrosis, shock and death
e.g. endotoxic shock: critical loss of blood pressure due to bacterial endotoxins (LPS)
Sterile solutions can contain LPS: bacteria dies in sterilization but LPS is unaltered
Due to serious consequences at very low levels of LPS, it is essential to test medical devices
and solutions for endotoxin
-Limulus Amoebocyte Lysate Assay: on horseshoe crab blood which contains amoebocytes
that will lyse and clot in the presence of extremely low levels of LPS
39.
PLASMIDS, LYSOGENY AND
PATHOGENICITY
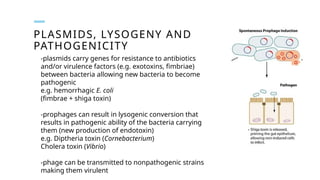
-plasmidscarry genes for resistance to antibiotics
and/or virulence factors (e.g. exotoxins, fimbriae)
between bacteria allowing new bacteria to become
pathogenic
e.g. hemorrhagic E. coli
(fimbrae + shiga toxin)
-prophages can result in lysogenic conversion that
results in pathogenic ability of the bacteria carrying
them (new production of endotoxin)
e.g. Diptheria toxin (Cornebacterium)
Cholera toxin (Vibrio)
-phage can be transmitted to nonpathogenic strains
making them virulent
40.
PATHOGENIC PROPERTIES OFVIRUS
1. Mechanisms to evade host defenses
A. Grow inside host cells to hide from immune defence
B. Kill immune cells
e.g. HIV – TH Cells
2. Cytopathic effects
= visible effects of viral infection on host cell: some effects will kill the cell, some will just
change the cell
A. stop DNA, RNA and/or protein synthesis
e.g. Herpes virus block mitosis
B. lysosomal autolysis of host cells
e.g. Influenza: bronchiolar epithelium
C. production of inclusion bodies (visible viral parts inside the cell)
can identify a particular virus
e.g. Rabies
41.
PATHOGENIC PROPERTIES OFVIRUS
D. syncytium formation (neighboring cells fuse together)
e.g. Varicella
E. change in cell function
e.g. Measles
F. production of interferons by host cell
(triggers host immune response)
G. induce antigenic changes on host cell surface (triggers destruction of
infected cell by host immune response)
H. induce chromosomal changes
I. cell transformation: may activate or deliver oncogenes resulting in loss of
contact inhibition (cancer)
e.g. Papilloma virus
42.
EUKARYOTIC PATHOGENS
1. Fungi:
-producetoxins causing allergies or disease
e.g. -chronic sinusitis (black molds)
-Stachybotrys: headaches, vomiting, mental disturbance
-invasive systemic mycosis in immune compromised patients
e.g. Candida
-mushrooms: mycotoxins may be hallucinogenic or deadly
43.
EUKARYOTIC PATHOGENS
2. Protozoa:
-cangrow inside host cells causing lysis
e.g. Malaria (Plasmodium)
-use host cells as food source
-produce wastes that cause disease
3. Algae
-produce neurotoxic substances
e.g. shellfish poisoning
(dinoflagellates)







![Lecture 6- Bacteria- Phathogenesis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture6-bacteria-phathogenesisautosaved-220830041321-bf3b2198-thumbnail.jpg?width=640&height=640&fit=bounds)



















































