Download to read offline


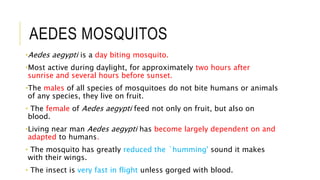


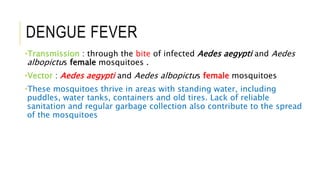
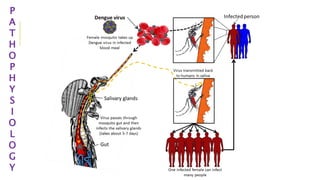
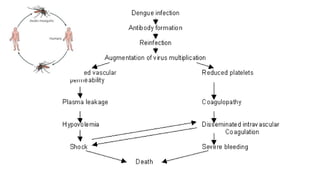
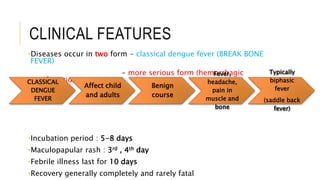
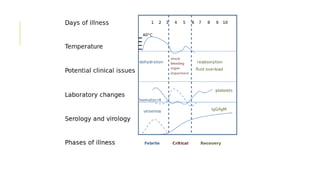
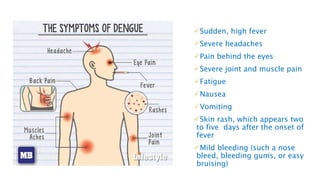


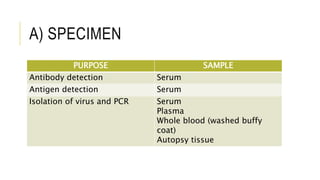





This document discusses dengue fever, a mosquito-borne viral disease. It defines dengue fever and lists its objectives which are to understand what dengue is, its risks, clinical features, epidemiology, laboratory diagnosis, treatment, and prophylaxis. It describes how dengue fever is transmitted through the bites of infected Aedes mosquitoes, mainly Aedes aegypti. The clinical features of dengue fever are explained including its rare, more serious forms like dengue hemorrhagic fever. The document outlines the laboratory tests used to diagnose dengue and the treatment which involves rest and pain relief medication. Controlling mosquito populations and developing a vaccine are discussed as important prophylaxis measures.























































































