Downloaded 23 times
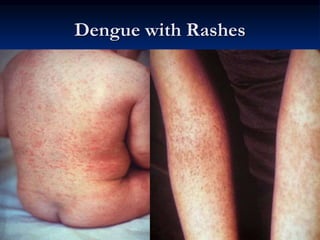



Dengue fever is caused by one of four dengue virus serotypes transmitted by Aedes mosquitoes. It is the most common arboviral infection worldwide, infecting 50-100 million people annually. There is no vaccine or antiviral treatment available, so prevention focuses on controlling mosquito populations. Symptoms range from flu-like illness to severe dengue hemorrhagic fever. Secondary infection with a different serotype increases the risk of more severe disease. Diagnosis involves virus isolation, serology to detect antibodies, or RT-PCR. Proper fluid management is critical for treating dengue hemorrhagic fever cases to reduce the risk of death.








































































