Download to read offline







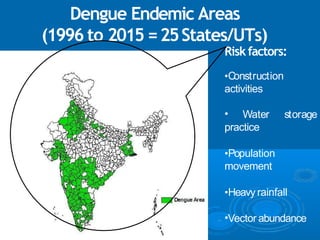








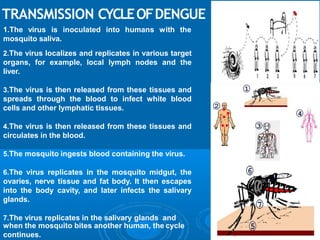





















Dengue is a viral disease transmitted by Aedes mosquitoes that is a major public health problem globally. It is endemic in over 100 countries and the distribution is comparable to malaria. There are four serotypes of the dengue virus. Dengue fever presents as a severe flu-like illness, while dengue hemorrhagic fever is a more severe form that can be fatal if untreated. Management involves treatment of symptoms, fluid replacement, monitoring for signs of plasma leakage, and blood transfusion if needed. Prevention relies on reducing mosquito breeding sites and personal protection against bites. Currently there is no vaccine for dengue.























































































