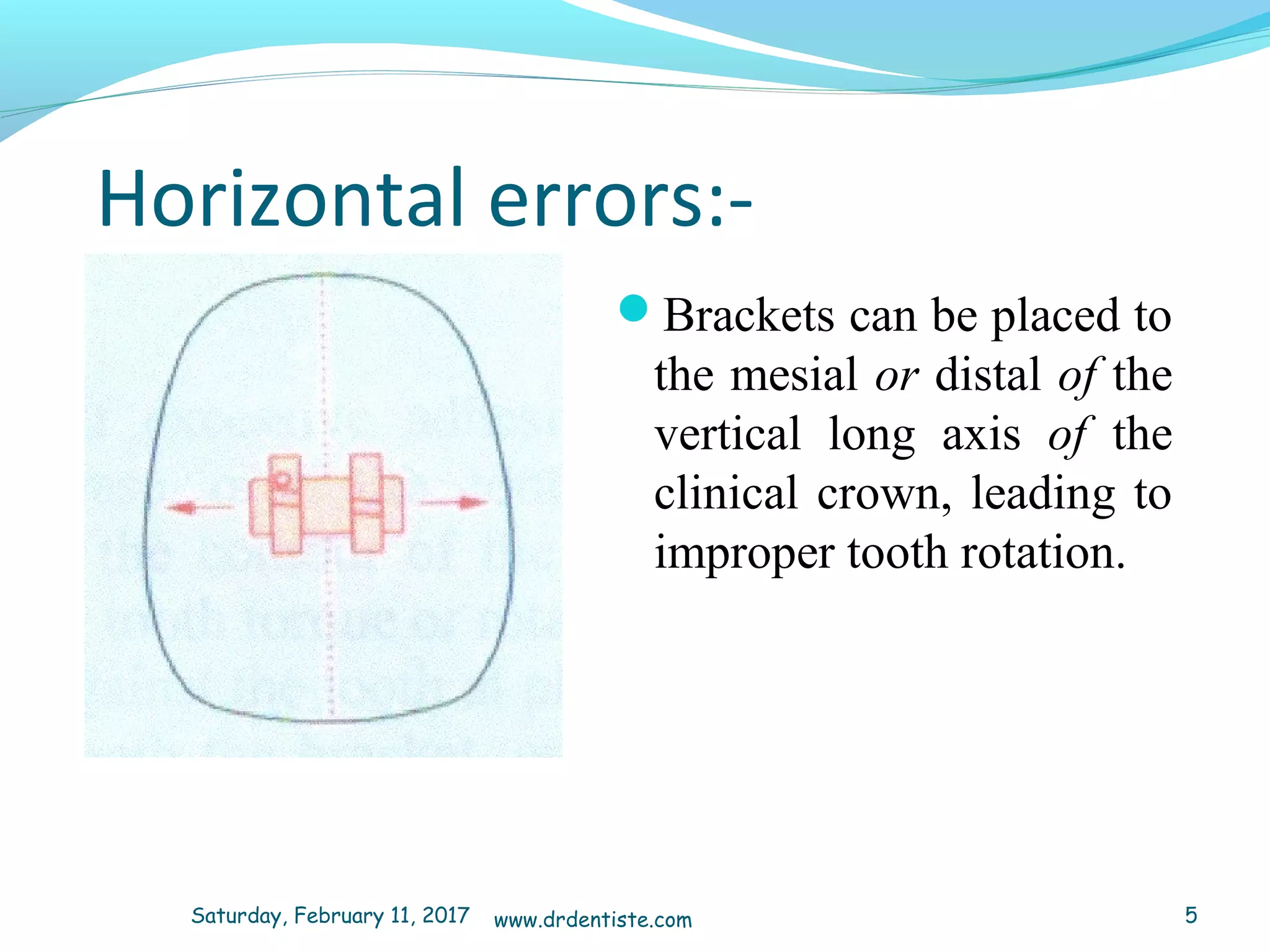
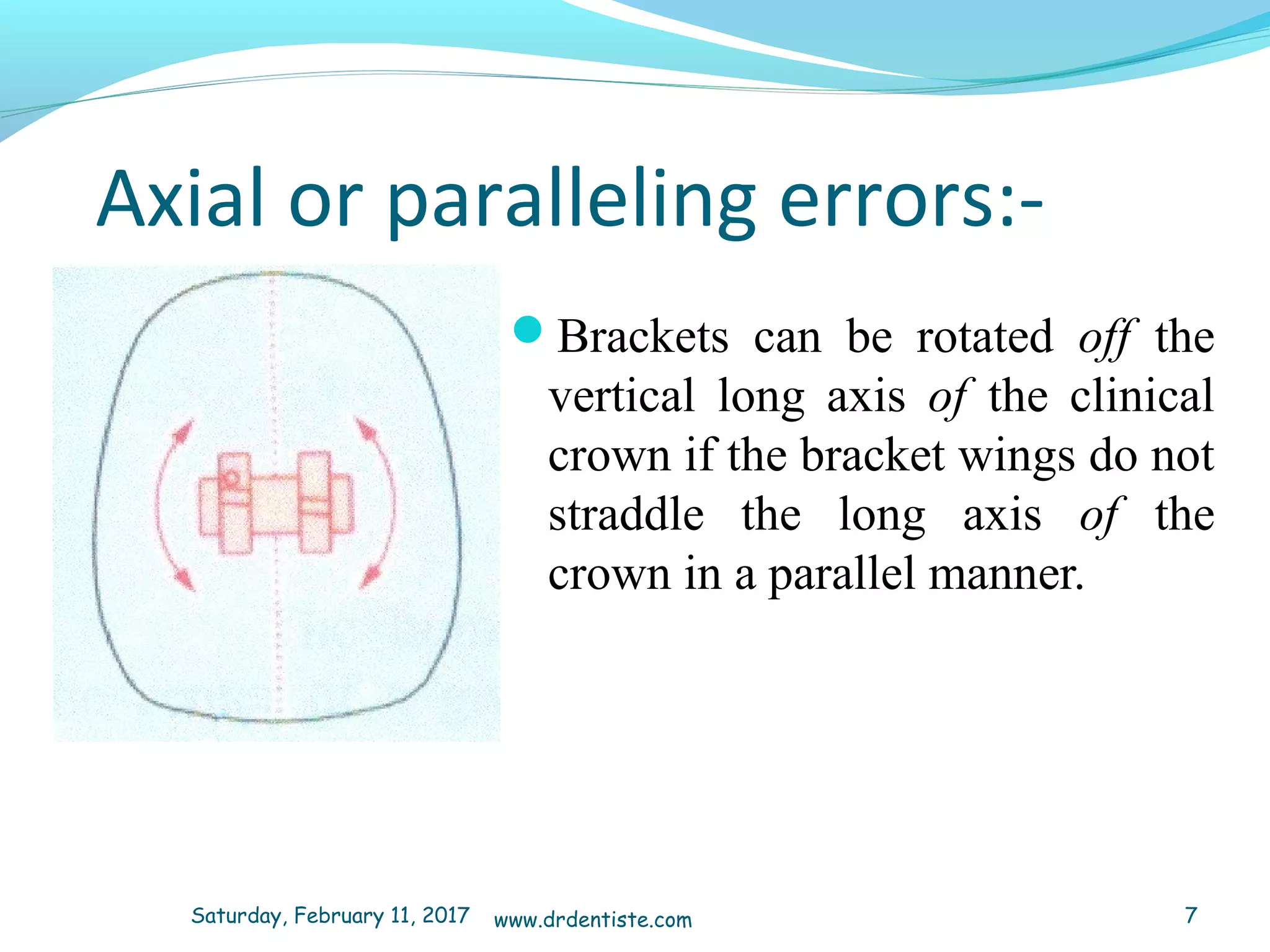
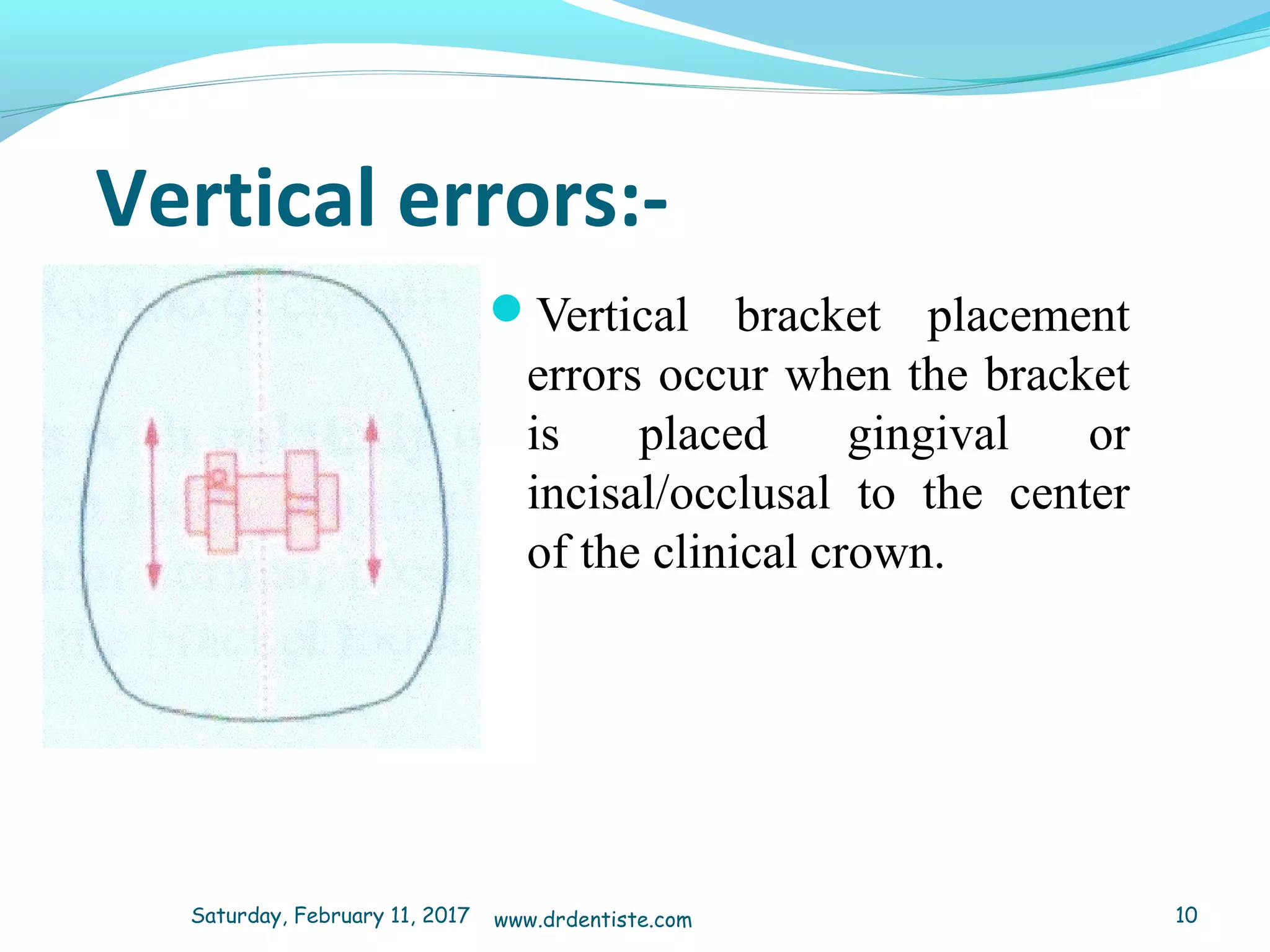
The document discusses methods for accurately placing orthodontic brackets on teeth. It describes potential errors in bracket placement including horizontal, axial, thickness, and vertical errors. It then discusses challenges in locating the center of clinical crowns for partially erupted teeth, teeth with gingival inflammation, teeth with displaced roots, or teeth with fractures or wear. The document proposes using a bracket placement chart to supplement direct visualization when placing brackets. The chart involves measuring crown heights, recording the values, selecting the closest row, and confirming bracket heights match the chart.