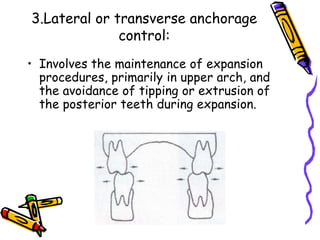
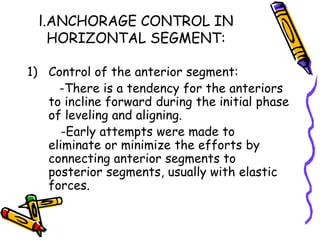
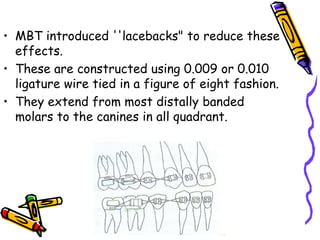
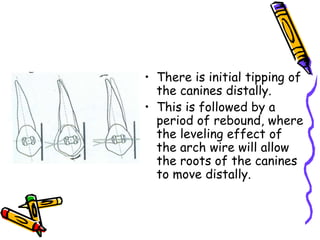
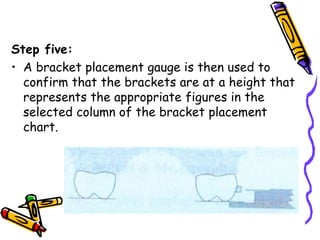
The document discusses Roth prescription and the development of the MBT bracket system. It describes how Roth observed that teeth will move after appliance removal and proposed overcorrection. This led to the development of the Roth prescription, which involves increased torque, tip, and in/out values compared to straightwire. The document then outlines how the MBT bracket system was developed by modifying the Roth prescription values based on new research. Key modifications included reduced anterior tip and lower posterior torque values. The document also discusses MBT bracket placement technique and methods for anchorage control.













![2.Vertical anchorage
control:
• Involves the need to try to
influence vertical skeletal &
dental development in the
posterior segment [as with
high angled cases] and at
times attempt to limit
vertical eruption of anterior
segments or even intrude
these segments.](https://image.slidesharecdn.com/rothprescription-230724153606-0deec4c2/85/Roth-prescription-ppt-69-320.jpg)