1. The maxillary sinus is an air-filled space within the body of the maxilla bone that communicates with the nasal cavity.
2. It develops from the 4th month of gestation and reaches its maximum size by 18 years of age.
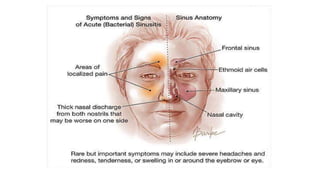
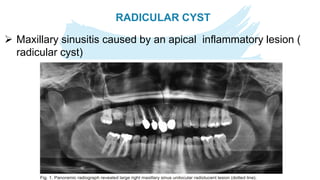
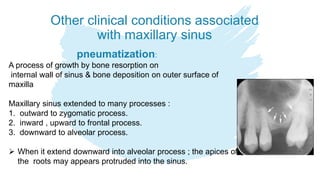
3. Common pathologies of the maxillary sinus include acute or chronic sinusitis, odontogenic cysts such as dentigerous or radicular cysts, and benign or malignant tumors.
4. Diagnostic evaluation of sinus disease involves medical history, clinical examination including transillumination, and radiographic imaging like panoramic radiograph, CT scan, or MRI.