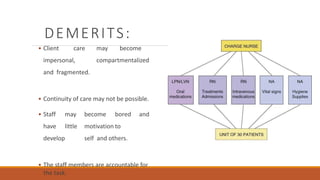
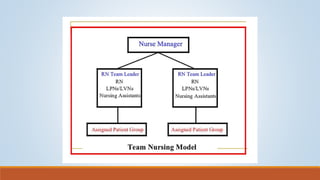
This document discusses various models for organizing nursing care delivery to patients. It describes case method, functional nursing, team nursing, modular nursing, progressive patient care, primary nursing, and case management models. For each model, it provides details on how care is organized and assigned, as well as the merits and demerits of each approach. It also discusses factors that influence quality of patient care and definitions of key terms like patient classification systems.