Nursing service aims to satisfy patient and community nursing needs. Placement involves assigning specific jobs, ranks, and responsibilities to candidates based on job requirements and qualifications. This improves employee outcomes like morale and turnover. Patient care is organized through assignment and delegation of duties among nursing personnel. Factors like patient characteristics and organizational support affect assignment patterns. Various nursing care delivery models distribute direct and indirect patient care functions among different roles.
Nursing service aims to meet the nursing needs of patients and the community.
Placement assigns specific jobs to candidates, improving morale, reducing turnover and absenteeism.
Assignment is the written delegation of duties. It defines systematic organization, cooperation, and accountability in nursing tasks.
Emphasizes coverage, quality, stability, and factors affecting assignment patterns including patient characteristics and nursing resources.
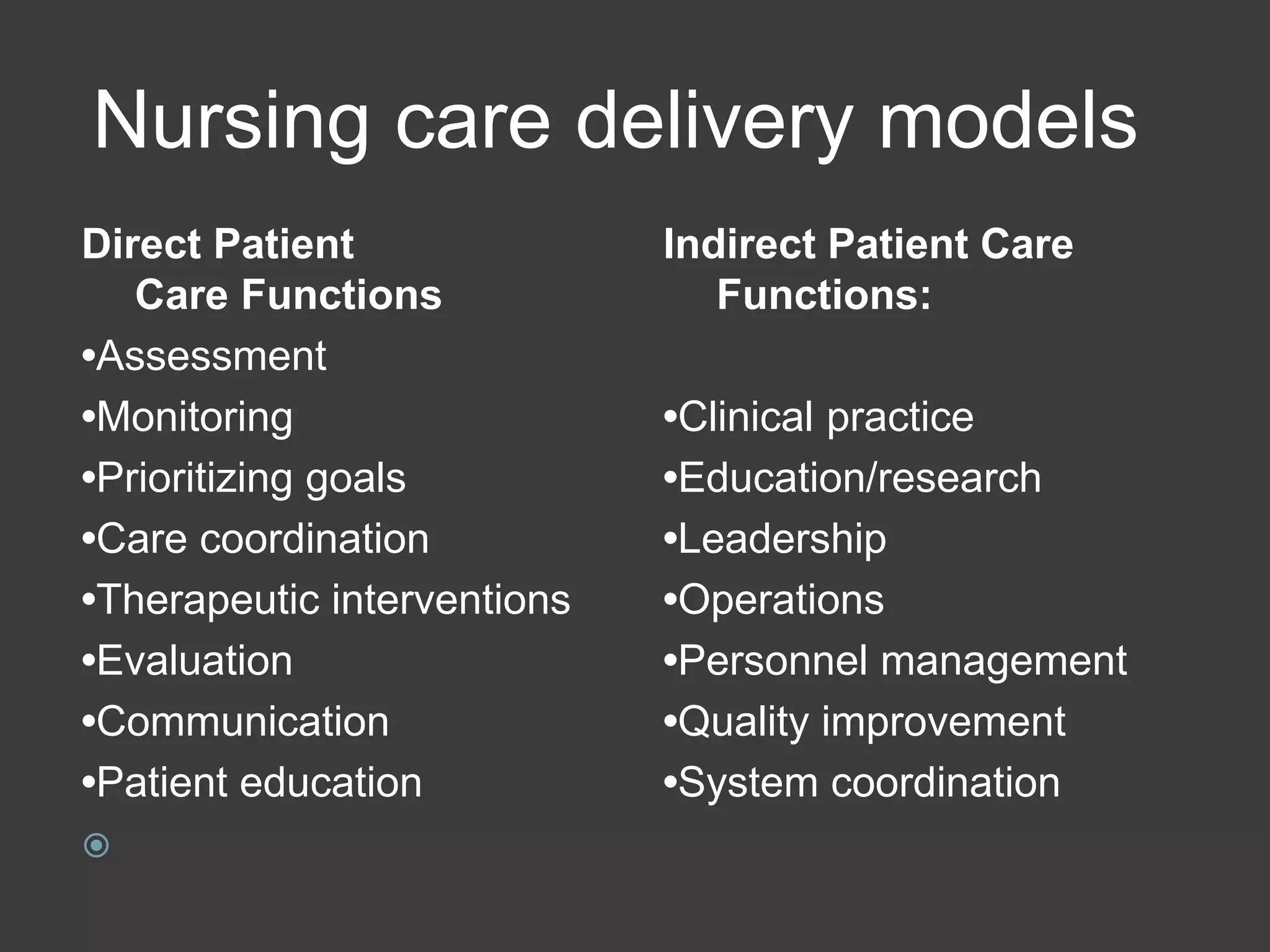
The models consist of direct (assessment, coordination) and indirect (leadership, management) patient care functions.
Planning and assignment are key processes for estimating nursing staff requirements based on bed numbers and patient dependency.
Considerations include teaching quality, staff morale, duty methods, calculations on nursing hours needed based on patient numbers.
Discusses patient classification systems that quantify nursing care requirements and how they match nursing resources to needs.
Categorizes care based on patient needs from self-care to intensive, outlining staffing ratios and requirements for each category.
Explores traditional methods like total patient care, case method and outlines advantages and disadvantages including autonomy and care fragmentation.
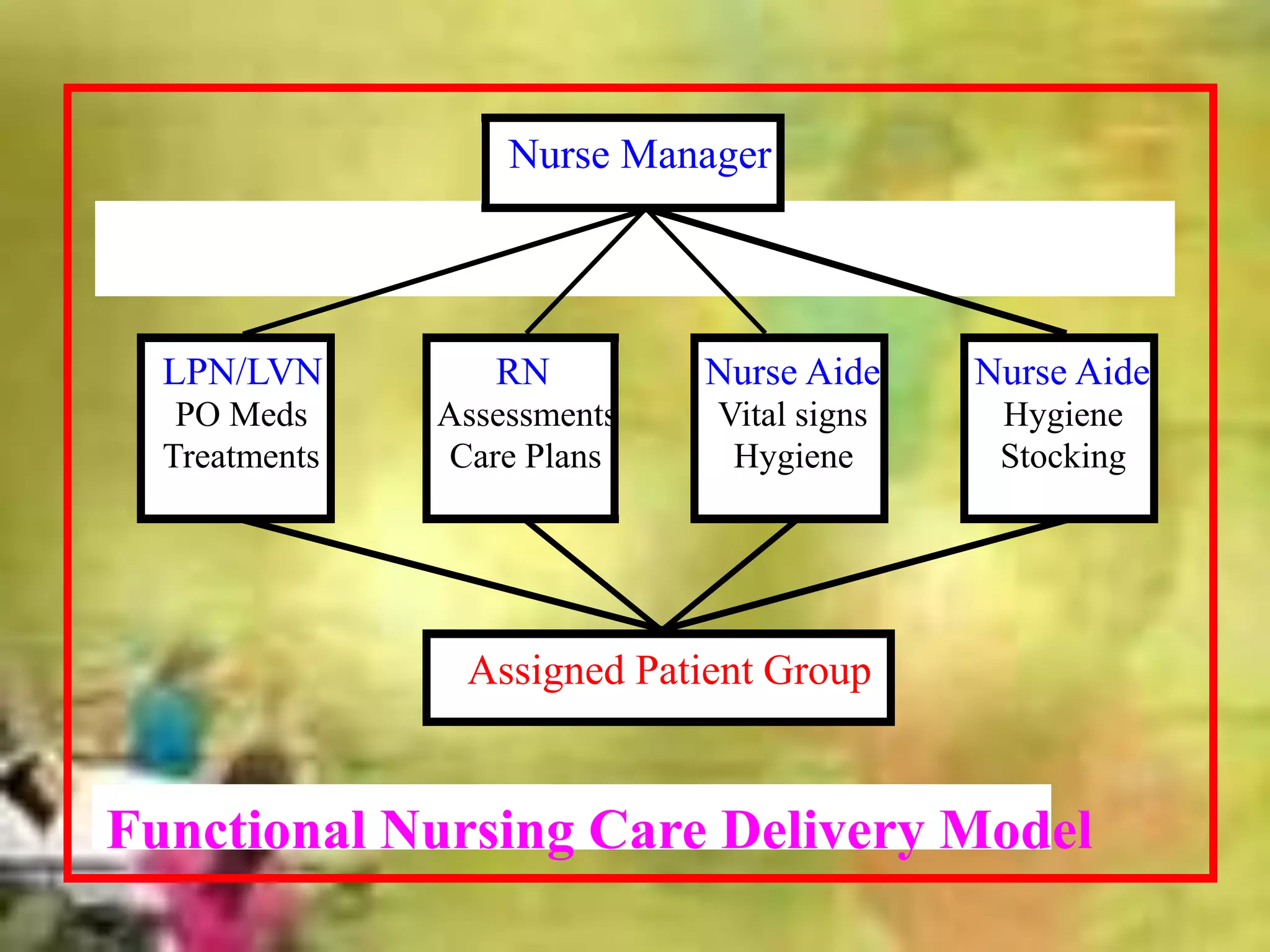
Describes functional nursing with defined roles, its advantages in efficiency, and challenges such as fragmented care.
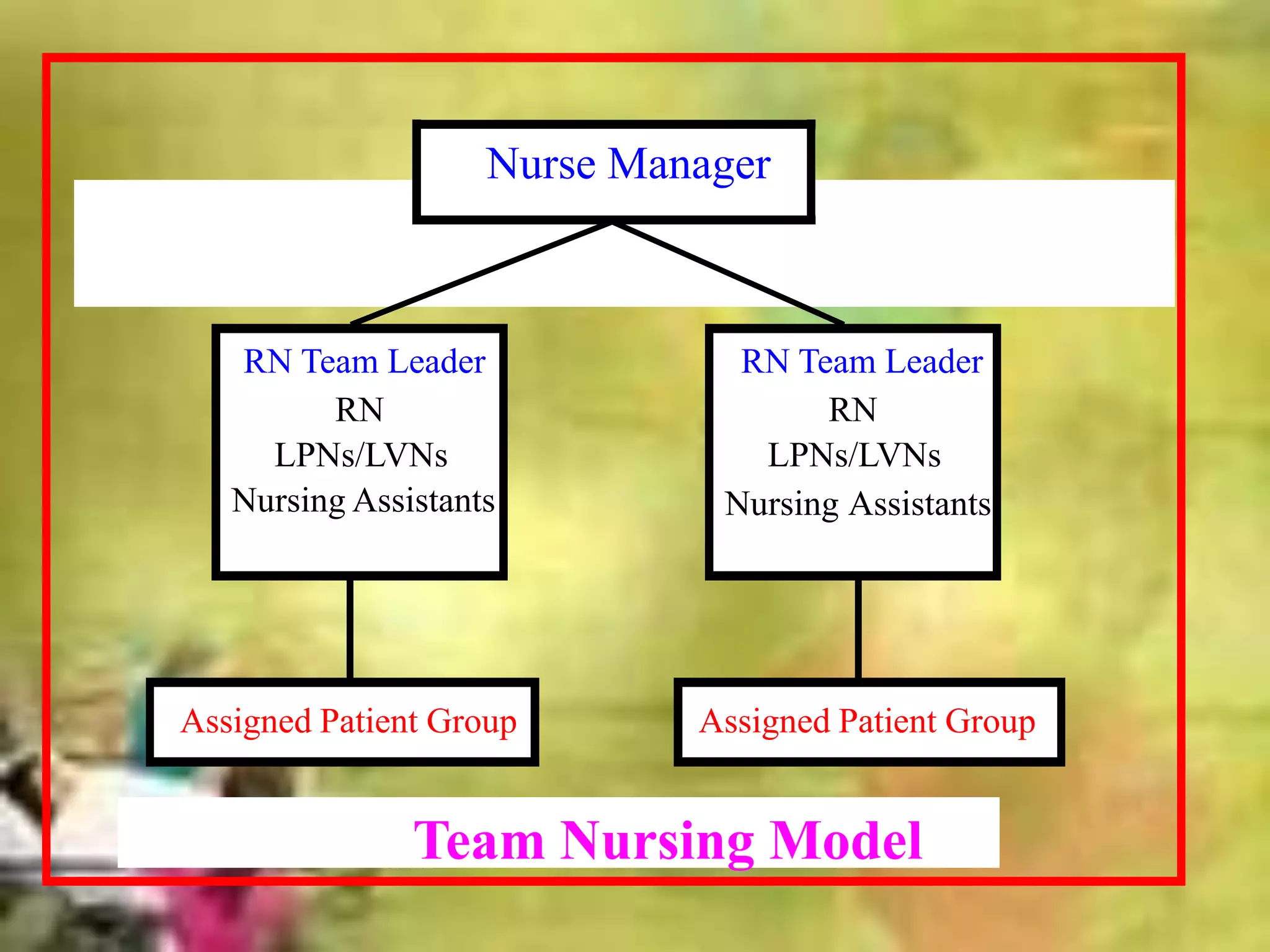
Team and modular nursing methods foster geographical organization, improved communication, and continuity of care.
Explains primary nursing, emphasizing 24-hour responsibility for patient care, highlighting both merits and challenges.
Case management coordinates patient care services through collaboration, ensuring health needs are met effectively.
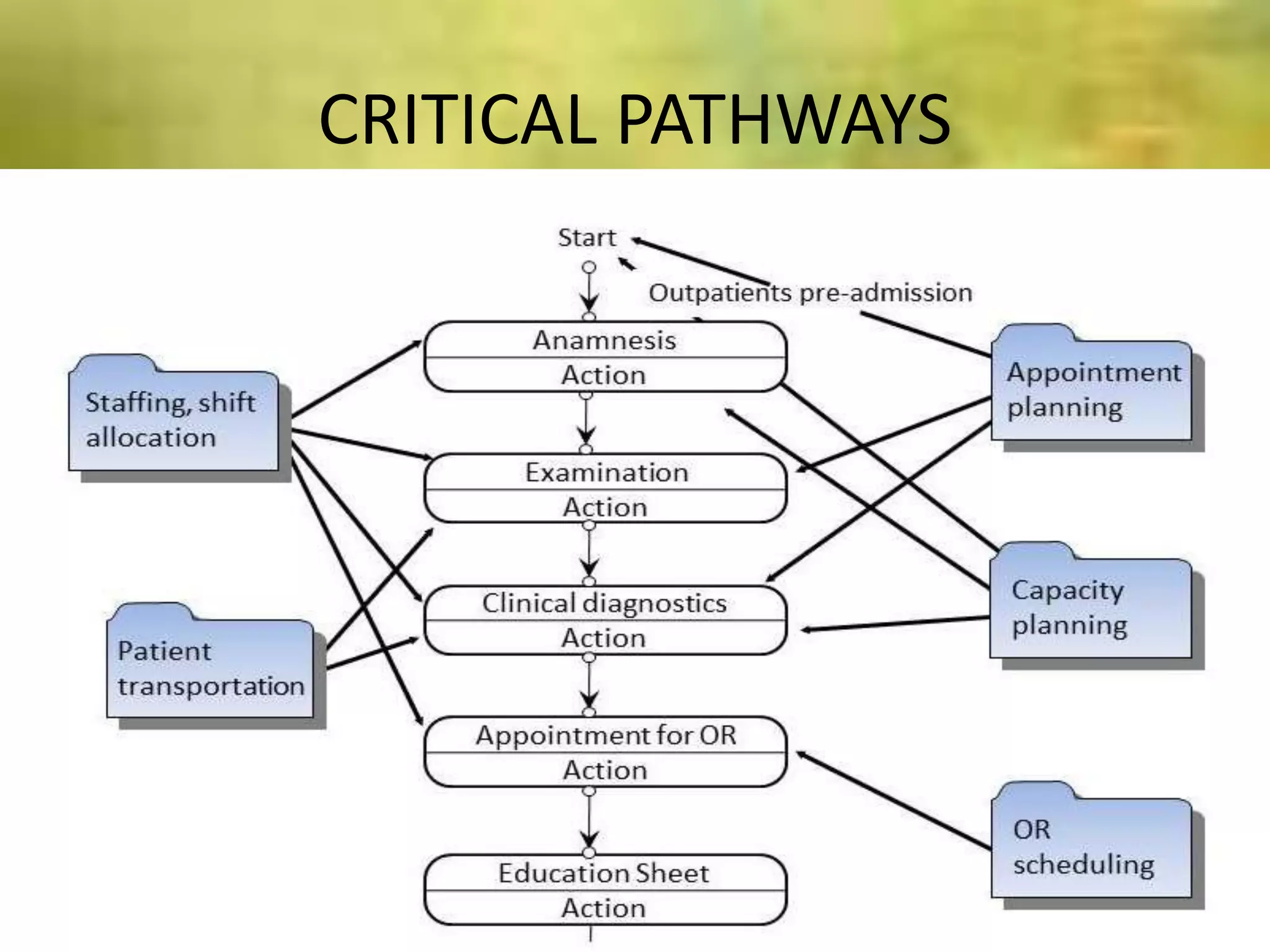
Discusses critical pathways, their advantages for standardized outcomes, and required competencies for case managers.Differentiated roles in nursing aim to align competencies with patient needs, promoting efficient resource use and job satisfaction.
Nurse managers supervise staff, assign duties, evaluate performance and face challenges like training needs and staffing shortages.
Summarizes relevant research on nurse-patient assignments and staffing levels associated with patient outcomes and case management.
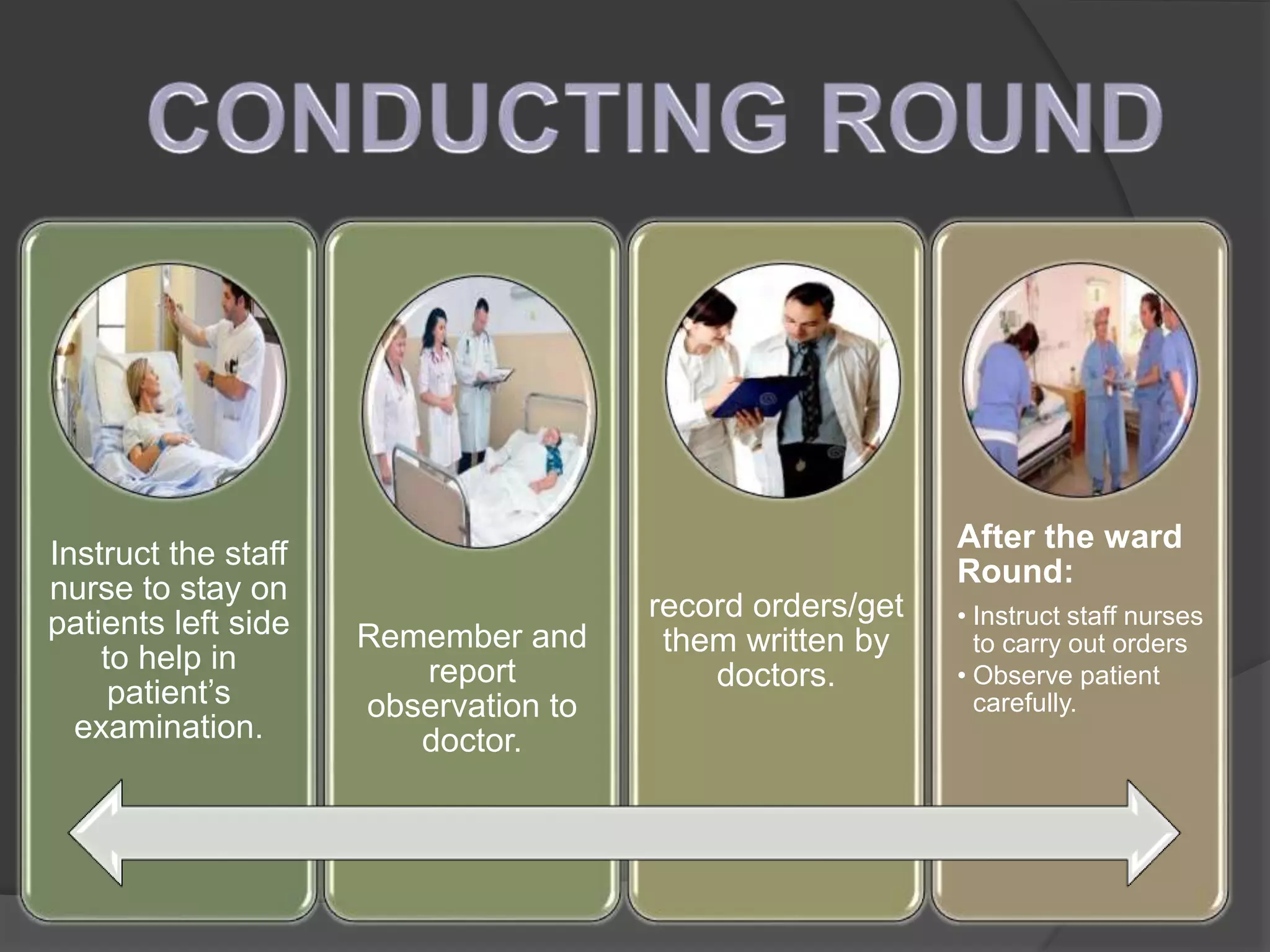
Instructs on daily nursing care protocols, emphasizing observations and proper execution of doctors' orders.
Nursing service isthe part of the
total health organization which
aims at satisfying the nursing
needs of the patients/
community.
3.
PLACEMENT-:
Placement is aprocess of assigning a
specific job to each of the selected
candidates. It involves assigning a specific
rank and responsibility to an individual. It
implies matching the requirements of a job
with the qualification of the candidate.
4.
It improves nurseemployee morale
It helps in reducing nurse employee turnover.
It helps in reducing absenteeism.
It helps in reducing accident rates.
It avoids the misfit between nurse and the job.
It helps the nurse to work for the pre determined objectives of the
organization.
5.
Assignment refers to“a written
delegation of duties to care for a
group of patients by trained
personnel assigned to the unit.”
6.
To delegate thework to be done to the nursing
personnel.
2- To gain the cooperation of the nursing personnel
by knowing and accepting the acceptance of the
work to be done.
3- To organize the work systematically.
4- To prepare and motivate the nurses for delivery
of care.
5- To shoulder accountability.
7.
Principles of personnelassignment:
Principles of personnel assignment:
1- Made by the head nurse or nurse in charge for each individual
nurse.
2- Based on:
a- Nursing needs of each patient and approximate time required to
care for him.
b- The capabilities, skill level, previous experience and the interest
of the staff members.
c- Job description.
3- Planned weekly, and revised daily if necessary to assure
continuity of care.
4- Take into account all the direct, indirect and unit activities
5- Consider the geographical location of the unit and the assigned
duties to save nurse’s time and effort.
6- Must be balanced among nursing staff.
7- Never to assign the same task to more than one nurse.
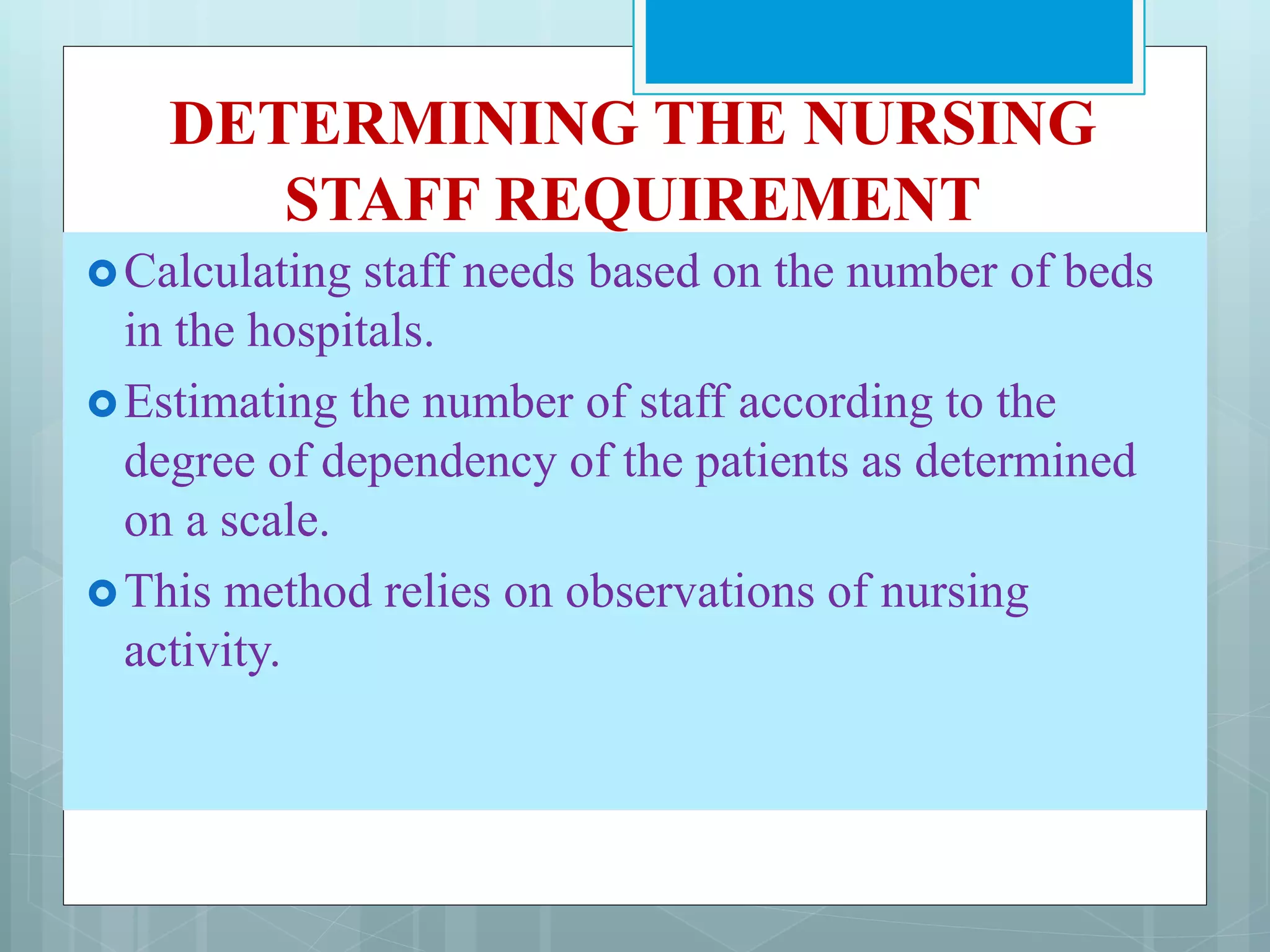
DETERMINING THE NURSING
STAFFREQUIREMENT
Calculating staff needs based on the number of beds
in the hospitals.
Estimating the number of staff according to the
degree of dependency of the patients as determined
on a scale.
This method relies on observations of nursing
activity.
15.
The amount andquality of teaching.
The amount and quality of supervision and
ward teaching.
The method of appointment of the medical staff.
The plan of ward floor plan.
The physical facilities.
16.
The amount,type and location of equipments and
supplies.
The number of working hours
The morale of the worker.
Methods of performing nursing procedures.
The time required for hospital routines
The method of assignment.
The standards of nursing care.
Good ward management.
18.
Guide tostaffing nursing services
1. Projecting Staffing Needs
Some steps to be taken in projecting staffing needs
include:
1. Identify the components of nursing care and nursing
service.
2. Define the standards of patient care to be maintained.
3. Estimate the average number of nursing hours needed
for the required hours.
4. Determine the proportion of nursing hours to be
provided by registered nurses and other nursing service
personnel
5. Determine polices regarding these positions and for
rotation of personnel.
19.
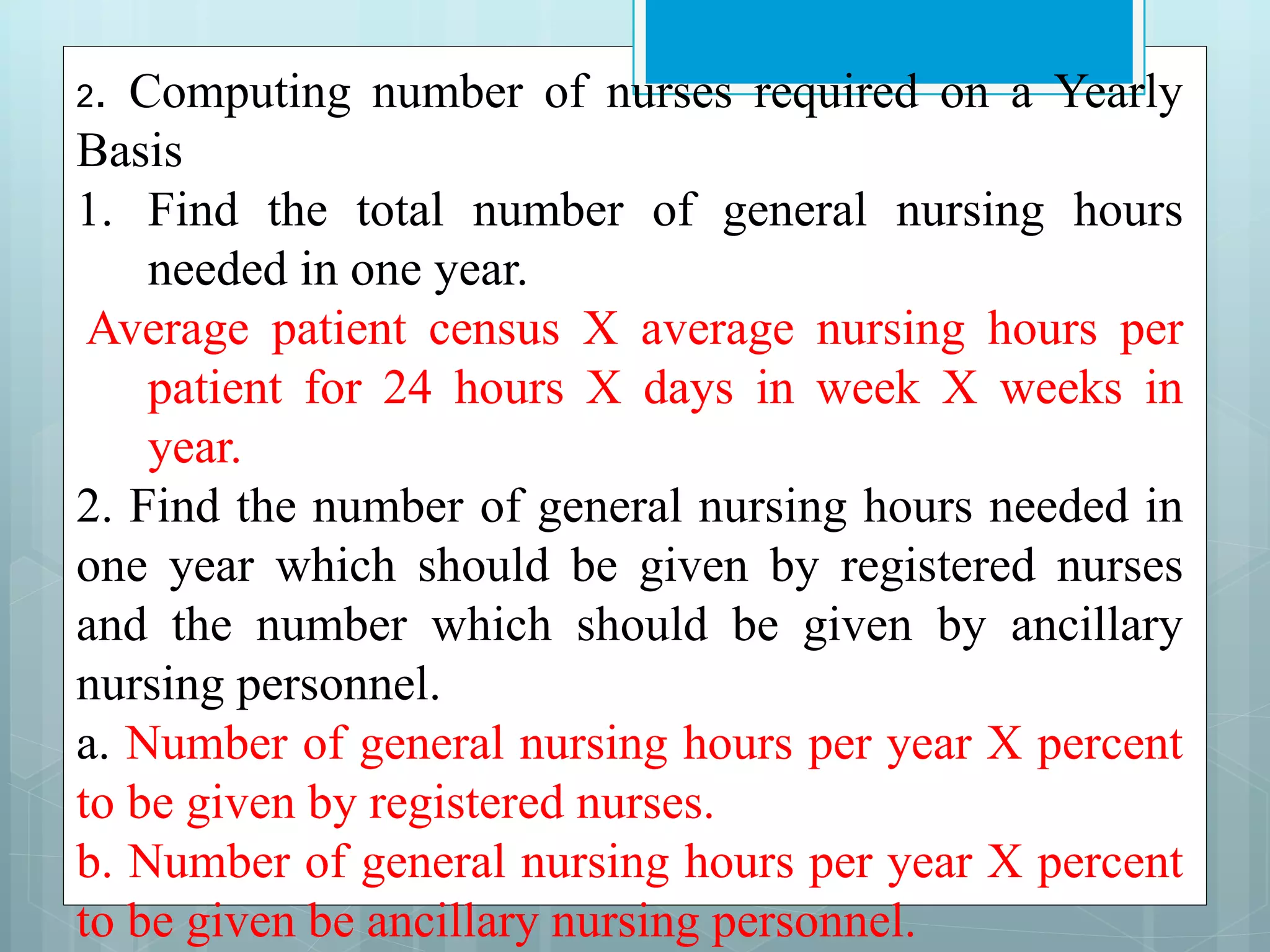
2. Computing numberof nurses required on a Yearly
Basis
1. Find the total number of general nursing hours
needed in one year.
Average patient census X average nursing hours per
patient for 24 hours X days in week X weeks in
year.
2. Find the number of general nursing hours needed in
one year which should be given by registered nurses
and the number which should be given by ancillary
nursing personnel.
a. Number of general nursing hours per year X percent
to be given by registered nurses.
b. Number of general nursing hours per year X percent
to be given be ancillary nursing personnel.
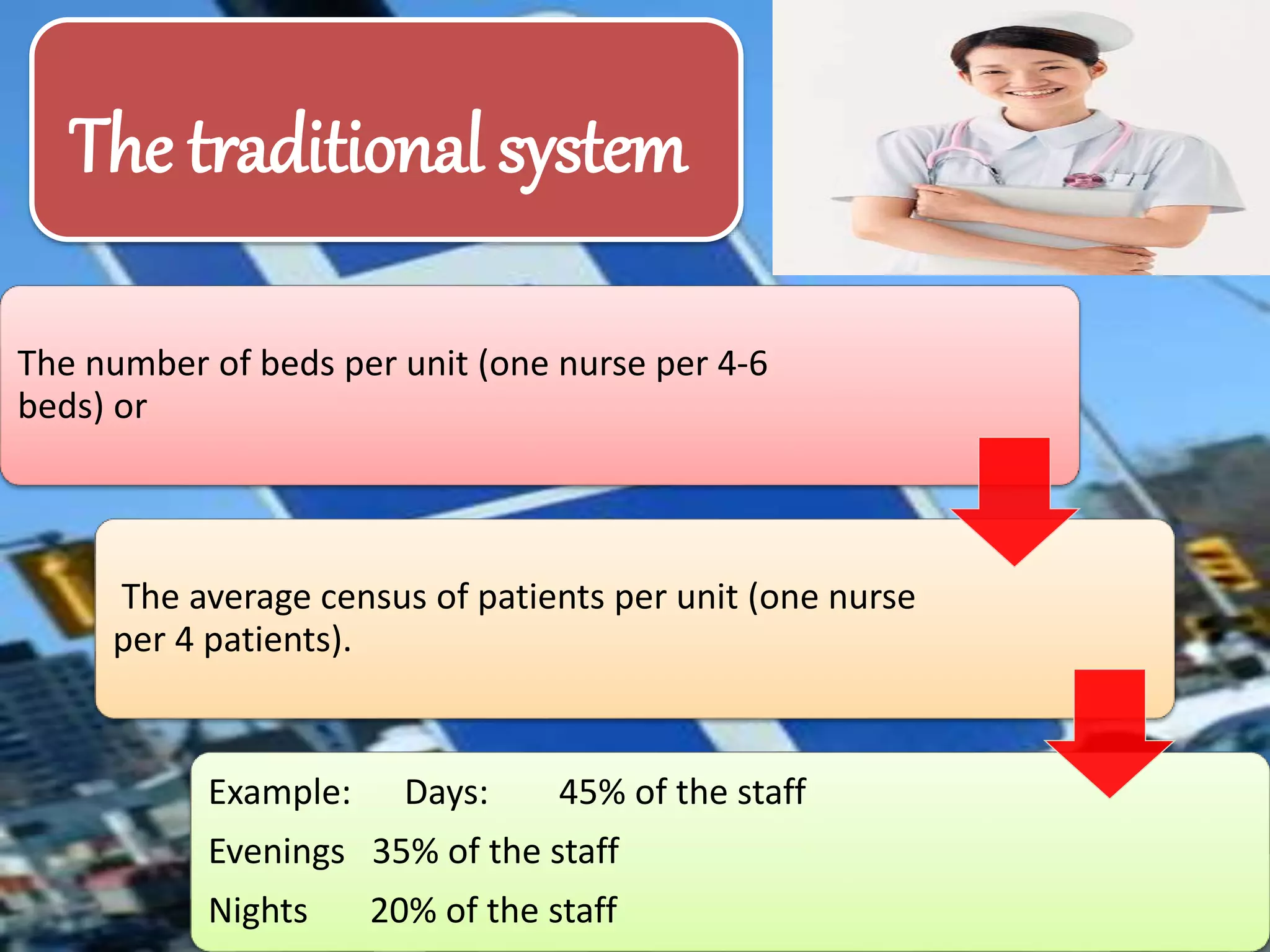
21.
The number ofbeds per unit (one nurse per 4-6
beds) or
The average census of patients per unit (one nurse
per 4 patients).
Example: Days: 45% of the staff
Evenings 35% of the staff
Nights 20% of the staff
The traditional system
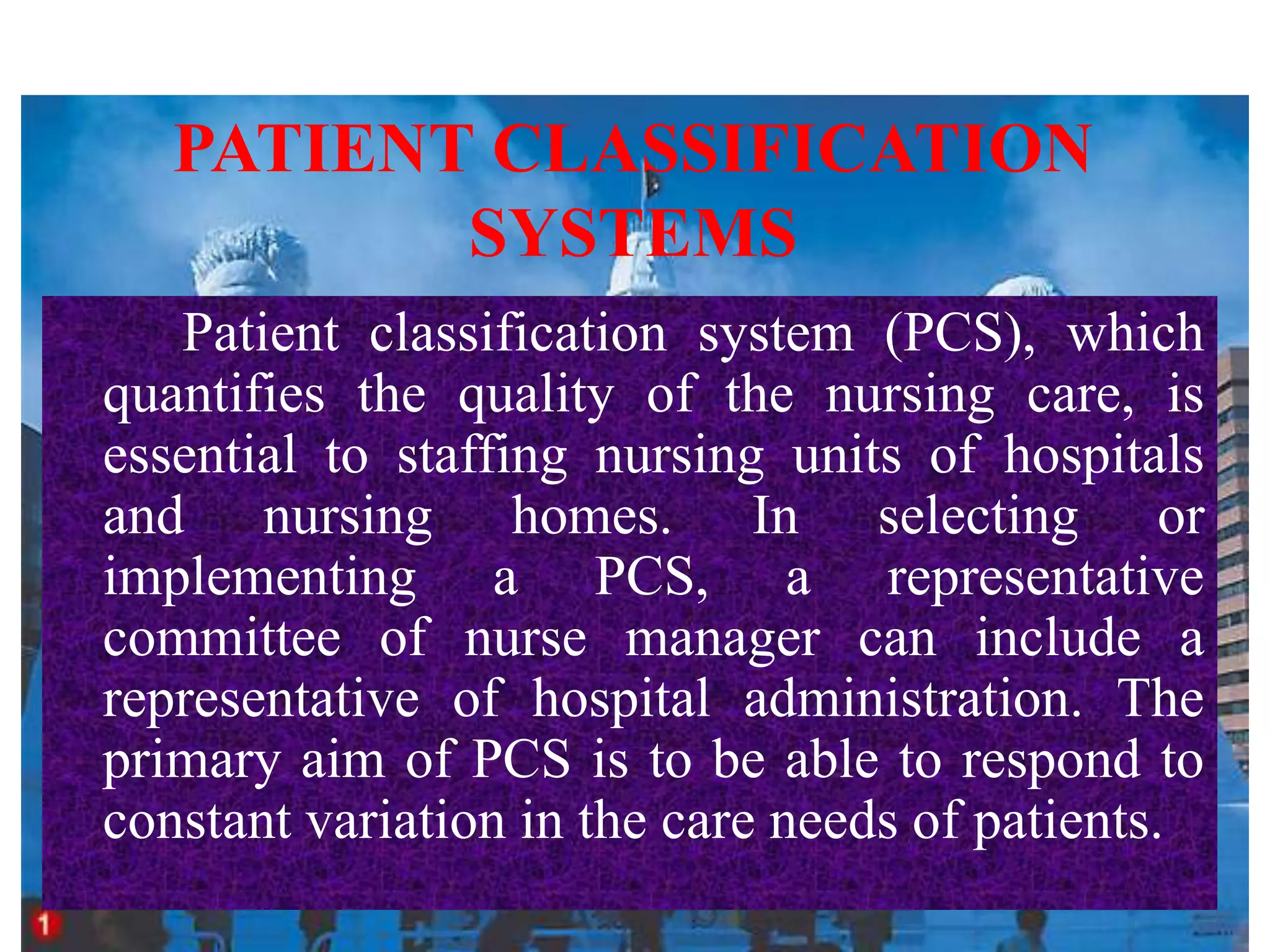
PATIENT CLASSIFICATION
SYSTEMS
Patient classificationsystem (PCS), which
quantifies the quality of the nursing care, is
essential to staffing nursing units of hospitals
and nursing homes. In selecting or
implementing a PCS, a representative
committee of nurse manager can include a
representative of hospital administration. The
primary aim of PCS is to be able to respond to
constant variation in the care needs of patients.
24.
Differentiate intensity ofcare among
definite classes.
Measure and quantify care to develop a
management engineering standard.
Match nursing resources to patient care
requirement.
Relate to time and effort spent on the
associated activity.
Be economical and convenient to repot and
use.
Characteristics
25.
Be mutually exclusive,continuing new item
under more than one unit.
Be open to audit.
Be understood by those who plan, schedule
and control the work.
Be individually standardized as to the
procedure needed for accomplishment.
Separate requirement for registered nurse
from those of other staff.
26.
PURPOSES
◘ The systemestablish a unit of
measure for nursing.
◘ Program costing and formulation
of the nursing budget.
◘ Tracking changes in patients care
needs.
◘ Determining the values of the
productivity equations
◘ Determine the quality
27.
TASK QUANTIFICATION.
Focuses onpatient needs.
The patients grouped according to their
nursing needs into 3 or more groups:
Group 1: Self care
Group 2: Partial or intermediate care
Group 3: Intensive or total care
28.
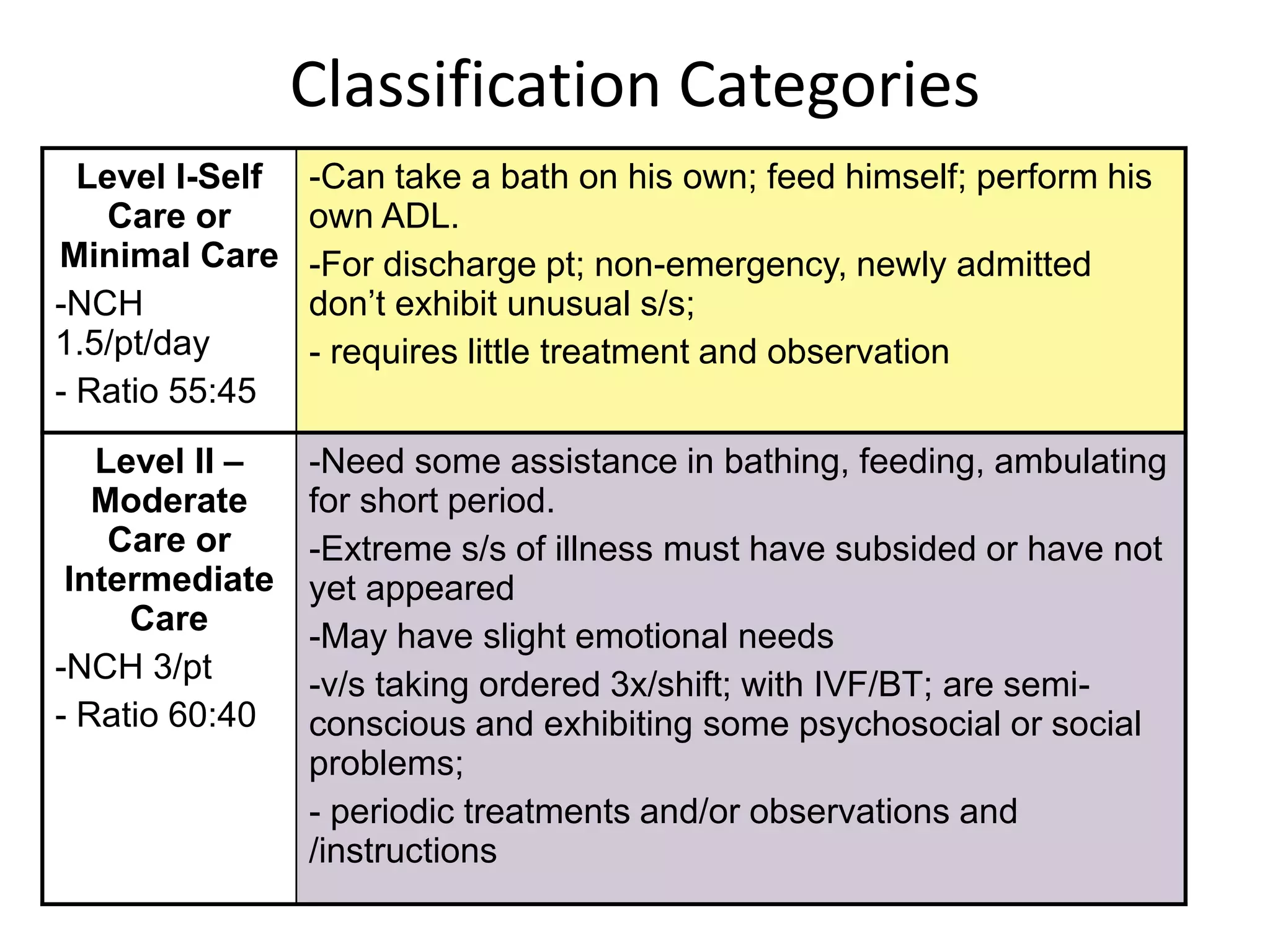
Classification Categories
Level I-Self
Careor
Minimal Care
-NCH
1.5/pt/day
- Ratio 55:45
-Can take a bath on his own; feed himself; perform his
own ADL.
-For discharge pt; non-emergency, newly admitted
don’t exhibit unusual s/s;
- requires little treatment and observation
Level II –
Moderate
Care or
Intermediate
Care
-NCH 3/pt
- Ratio 60:40
-Need some assistance in bathing, feeding, ambulating
for short period.
-Extreme s/s of illness must have subsided or have not
yet appeared
-May have slight emotional needs
-v/s taking ordered 3x/shift; with IVF/BT; are semi-
conscious and exhibiting some psychosocial or social
problems;
- periodic treatments and/or observations and
/instructions
29.
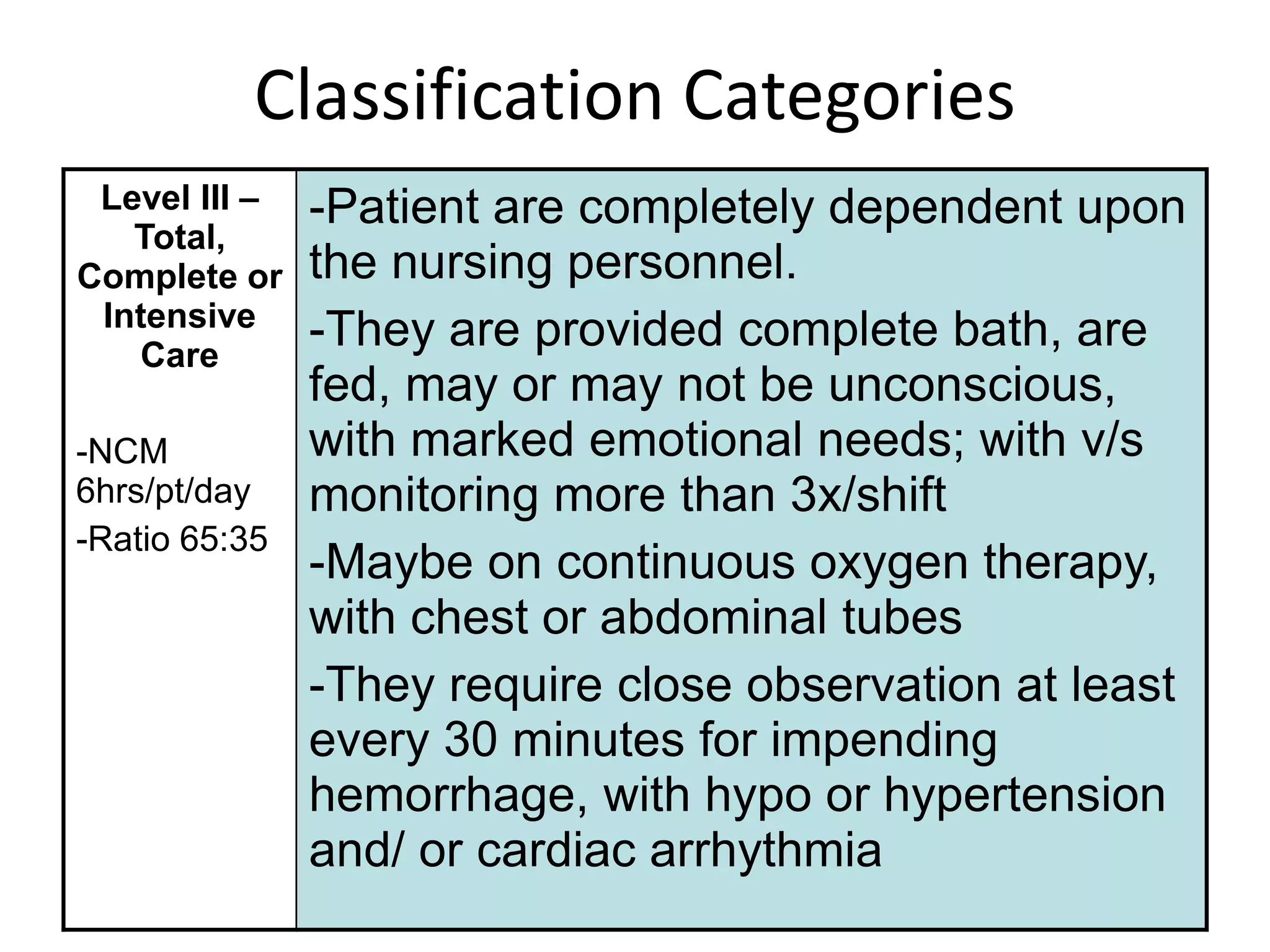
Classification Categories
Level III–
Total,
Complete or
Intensive
Care
-NCM
6hrs/pt/day
-Ratio 65:35
-Patient are completely dependent upon
the nursing personnel.
-They are provided complete bath, are
fed, may or may not be unconscious,
with marked emotional needs; with v/s
monitoring more than 3x/shift
-Maybe on continuous oxygen therapy,
with chest or abdominal tubes
-They require close observation at least
every 30 minutes for impending
hemorrhage, with hypo or hypertension
and/ or cardiac arrhythmia
30.
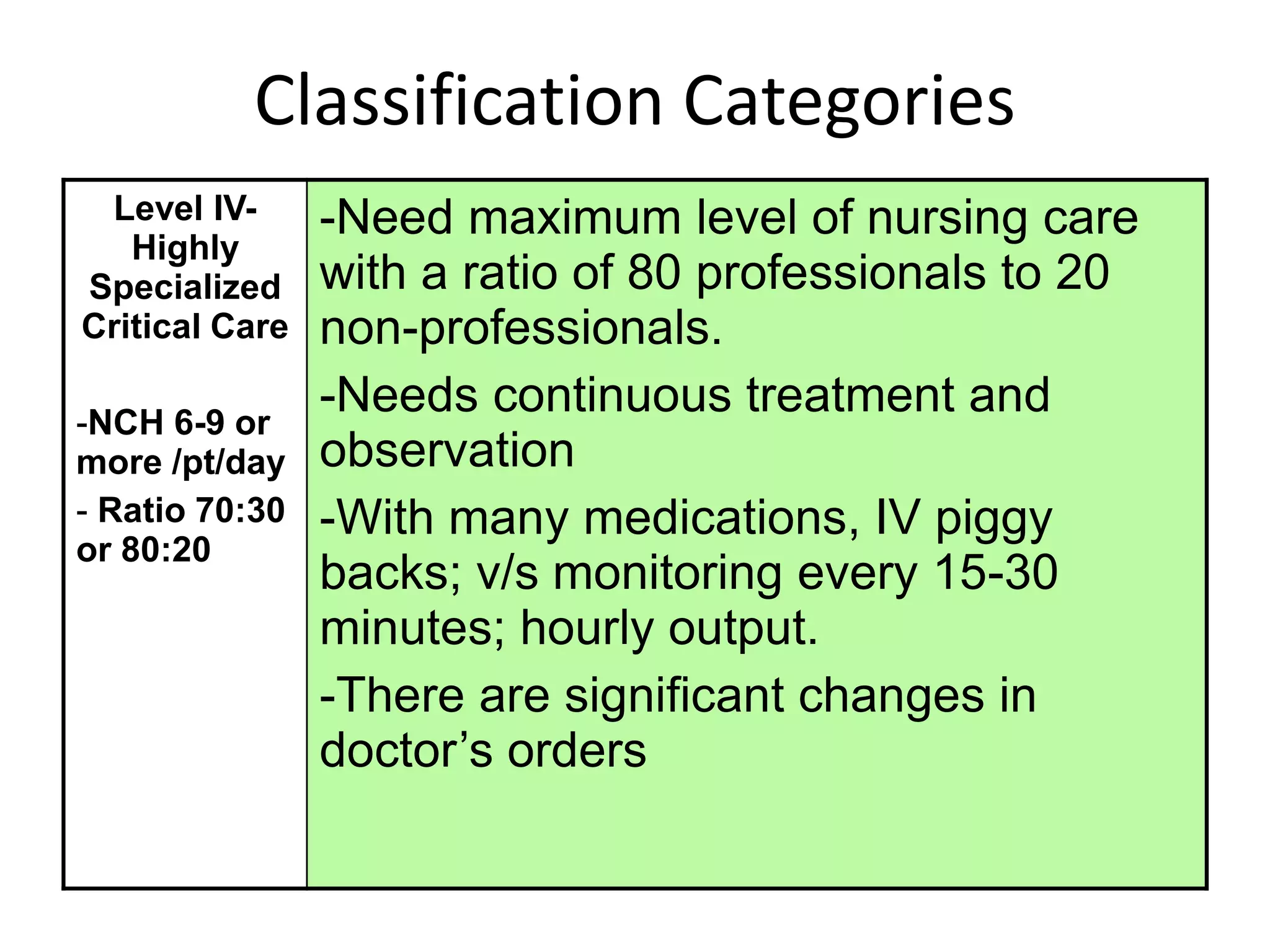
Classification Categories
Level IV-
Highly
Specialized
CriticalCare
-NCH 6-9 or
more /pt/day
- Ratio 70:30
or 80:20
-Need maximum level of nursing care
with a ratio of 80 professionals to 20
non-professionals.
-Needs continuous treatment and
observation
-With many medications, IV piggy
backs; v/s monitoring every 15-30
minutes; hourly output.
-There are significant changes in
doctor’s orders
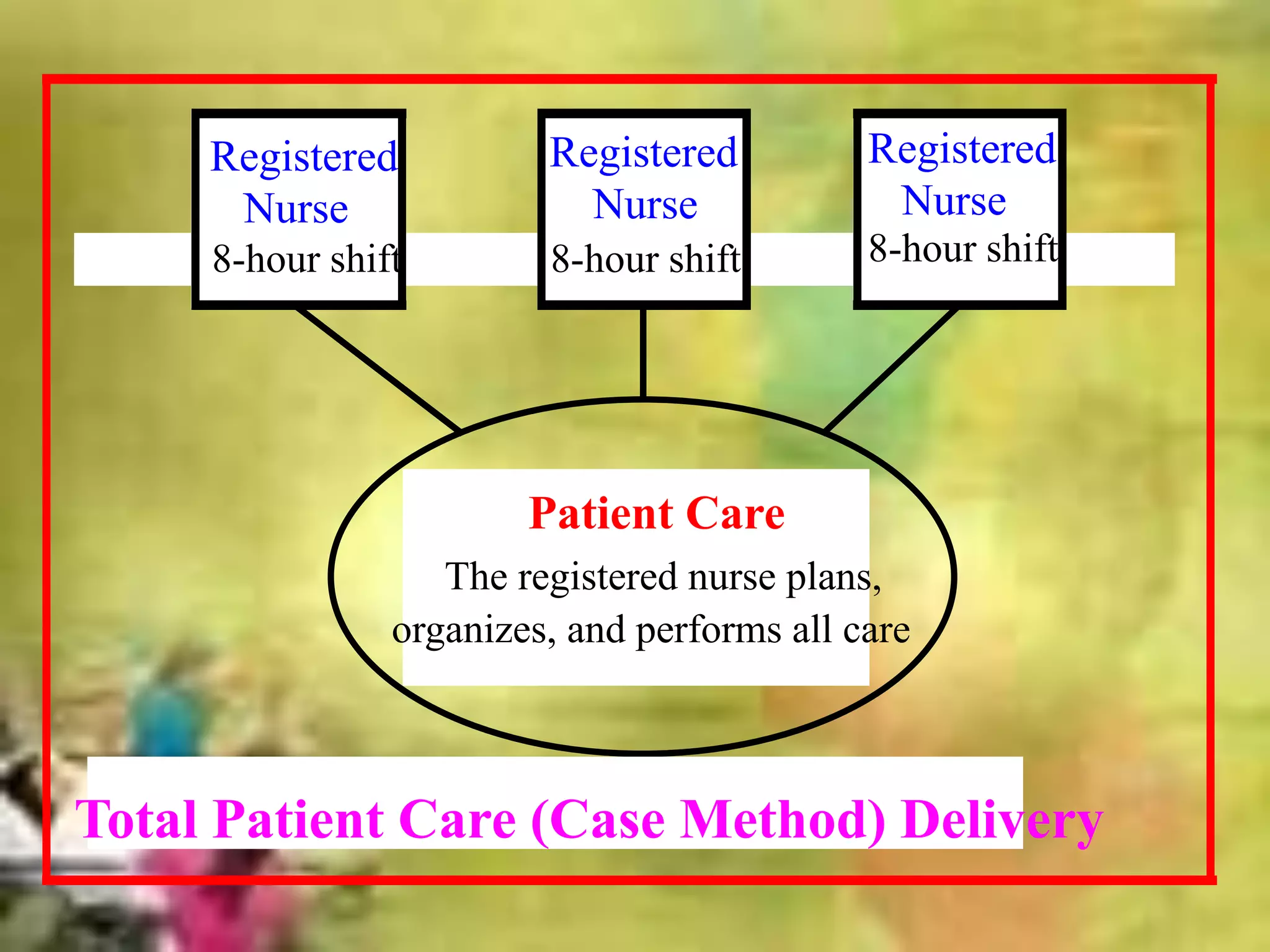
Patient Care
The registerednurse plans,
organizes, and performs all care
Registered
Nurse
8-hour shift
Registered
Nurse
8-hour shift
Registered
Nurse
8-hour shift
Total Patient Care (Case Method) Delivery
34.
one professional nurse
assumestotal
responsibility of
providing complete
care for one or more
patients (1-6) while
she is on duty. This
method is used
frequently in intensive
care units and in
teaching nursing
35.
• Advantages
• Highdegree of autonomy
• Lines of responsibility and accountability are
clear
• Patient receives holistic, unregimented care
• Disadvantages
• Each RN may have a different approach to care
• Not cost-effective
• Lack of RN availability
Advantages:
•Care is providedeconomically and
efficiently
•Minimum number of RNs required, so it is
efficient when there is a shortage in the
staff or there is limited number of
professional nurses
•Tasks are completed quickly
•Useful in emergency situations.
38.
Disadvantages:
Care may befragmented
Patient may be confused with many care
providers
Caregivers feel unchallenged
Lack of communication among the different
persons who care for the patient.
Neglecting the humanity of the patient and
the individual needs of the patient will be los
in an effort to get the work done.
39.
Nurse Manager
RN TeamLeader
RN
LPNs/LVNs
Nursing Assistants
RN Team Leader
RN
LPNs/LVNs
Nursing Assistants
Assigned Patient Group Assigned Patient Group
Team Nursing Model
40.
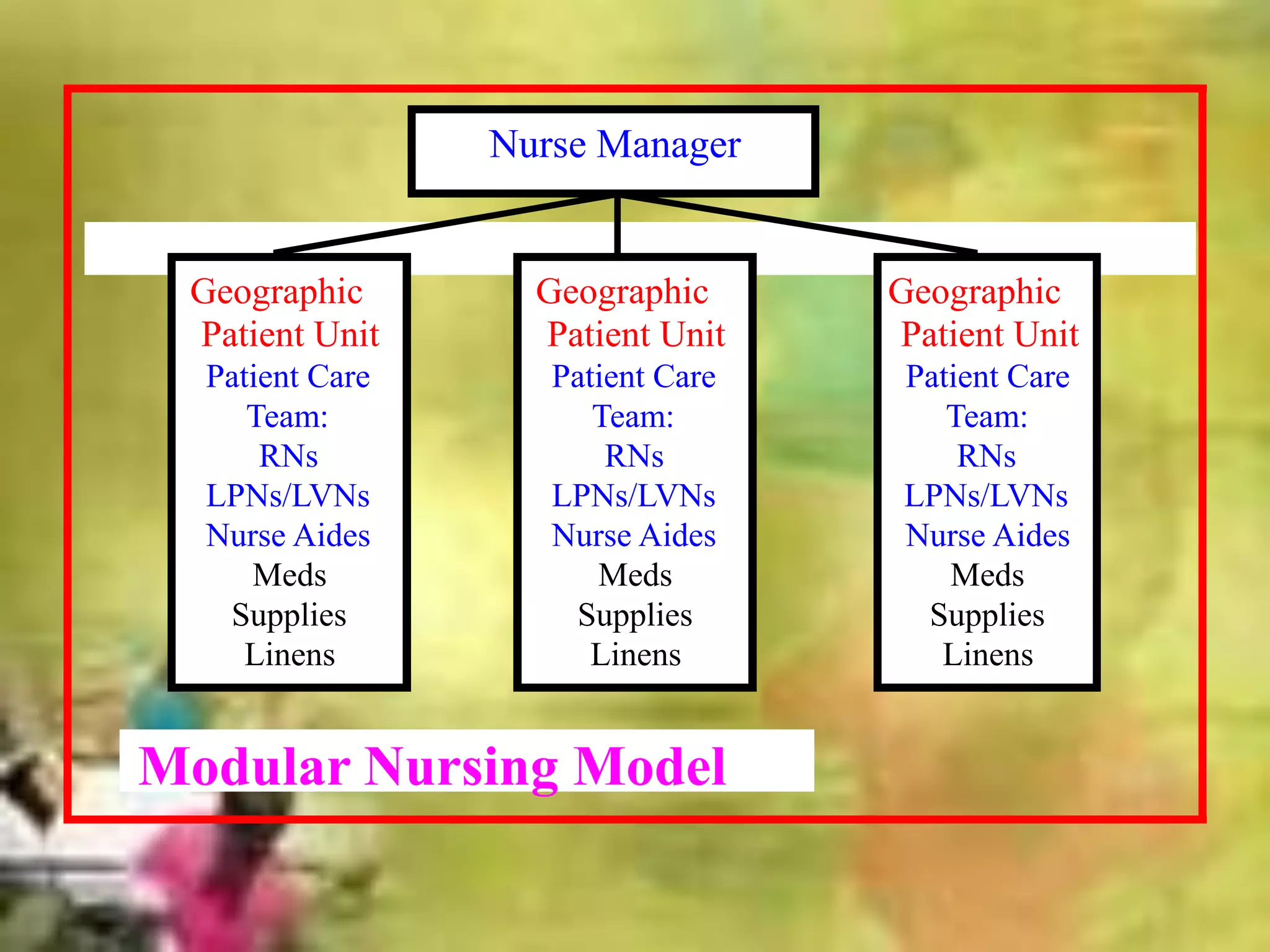
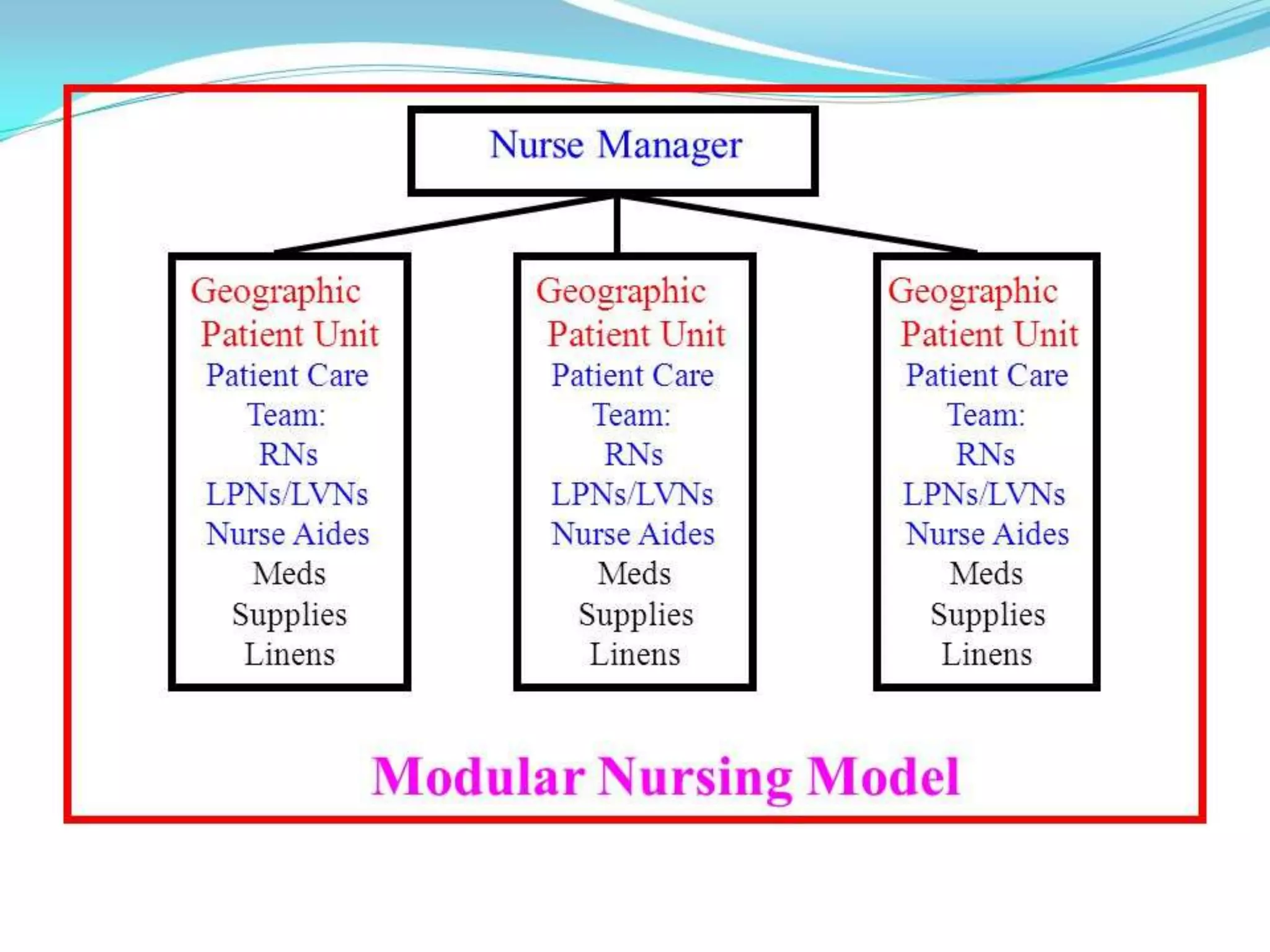
Geographic
Patient Unit
Patient Care
Team:
RNs
LPNs/LVNs
NurseAides
Meds
Supplies
Linens
Geographic
Patient Unit
Patient Care
Team:
RNs
LPNs/LVNs
Nurse Aides
Meds
Supplies
Linens
Geographic
Patient Unit
Patient Care
Team:
RNs
LPNs/LVNs
Nurse Aides
Meds
Supplies
Linens
Nurse Manager
Modular Nursing Model
41.
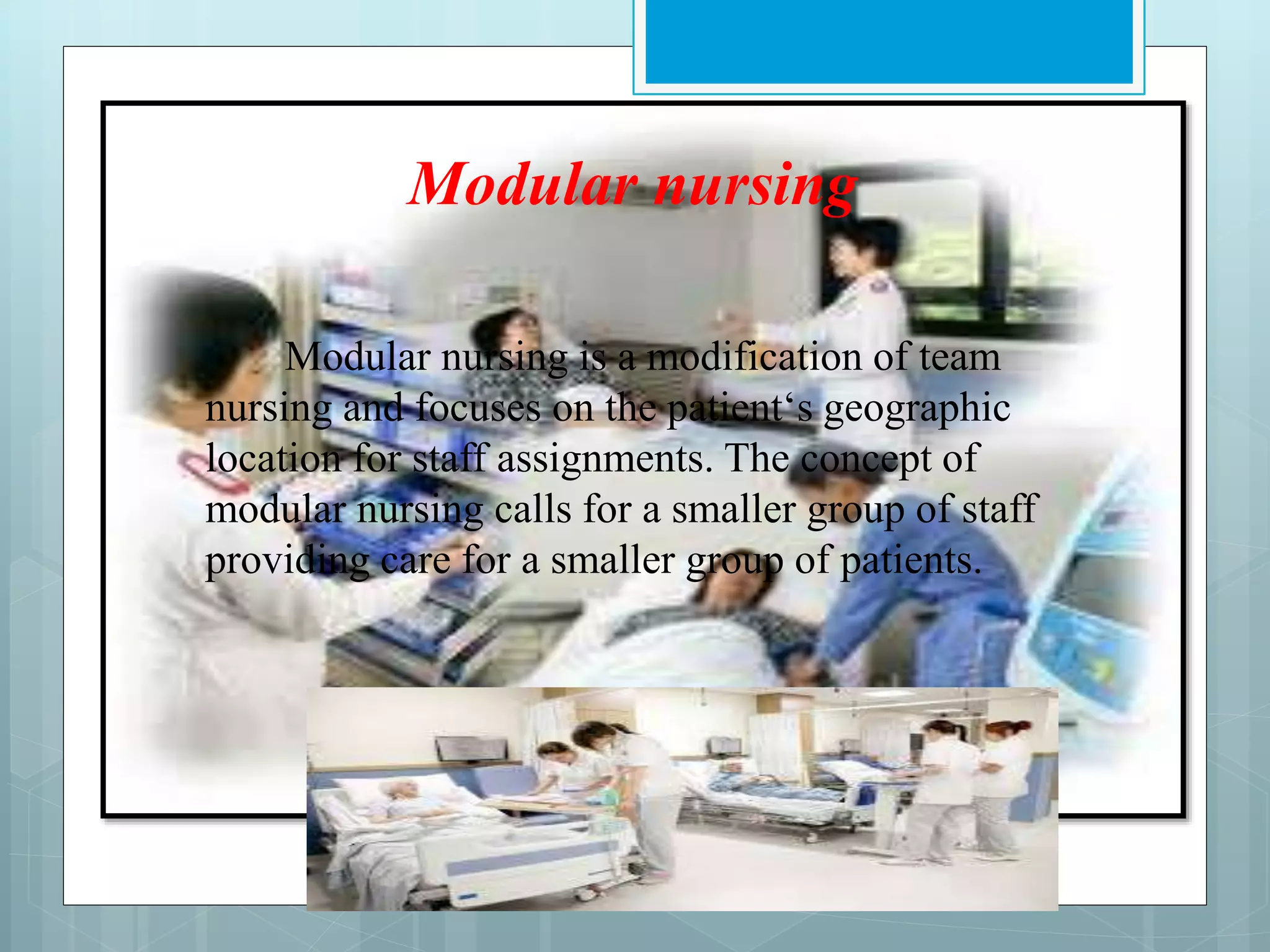
Modular nursing
Modular nursingis a modification of team
nursing and focuses on the patient‘s geographic
location for staff assignments. The concept of
modular nursing calls for a smaller group of staff
providing care for a smaller group of patients.
43.
. MODULAR NURSING:
Modularnursing assignment is used when the
nursing staff includes technical and nurse aides,
as well as professional nurses. Although two or
three persons are assigned to each module, the
greatest responsibility for the care of assigned
patients falls on the professional nurse. The
professional nurse is also responsible for guiding
and teaching non-professional nurse.
44.
Advantages
Continuity ofcare is improved.
RN more involved in planning and
coordinating care.
Geographic closeness and efficient
communication.
Disadvantages
Increased costs to stock each module.
Long corridors not conducive to modular
nursing.
45.
Primary nursing:
Itis also called relationship based nursing. It
involves total nursing care, directed by a nurse on
24 hour basis as long as the client is under the
care.
46.
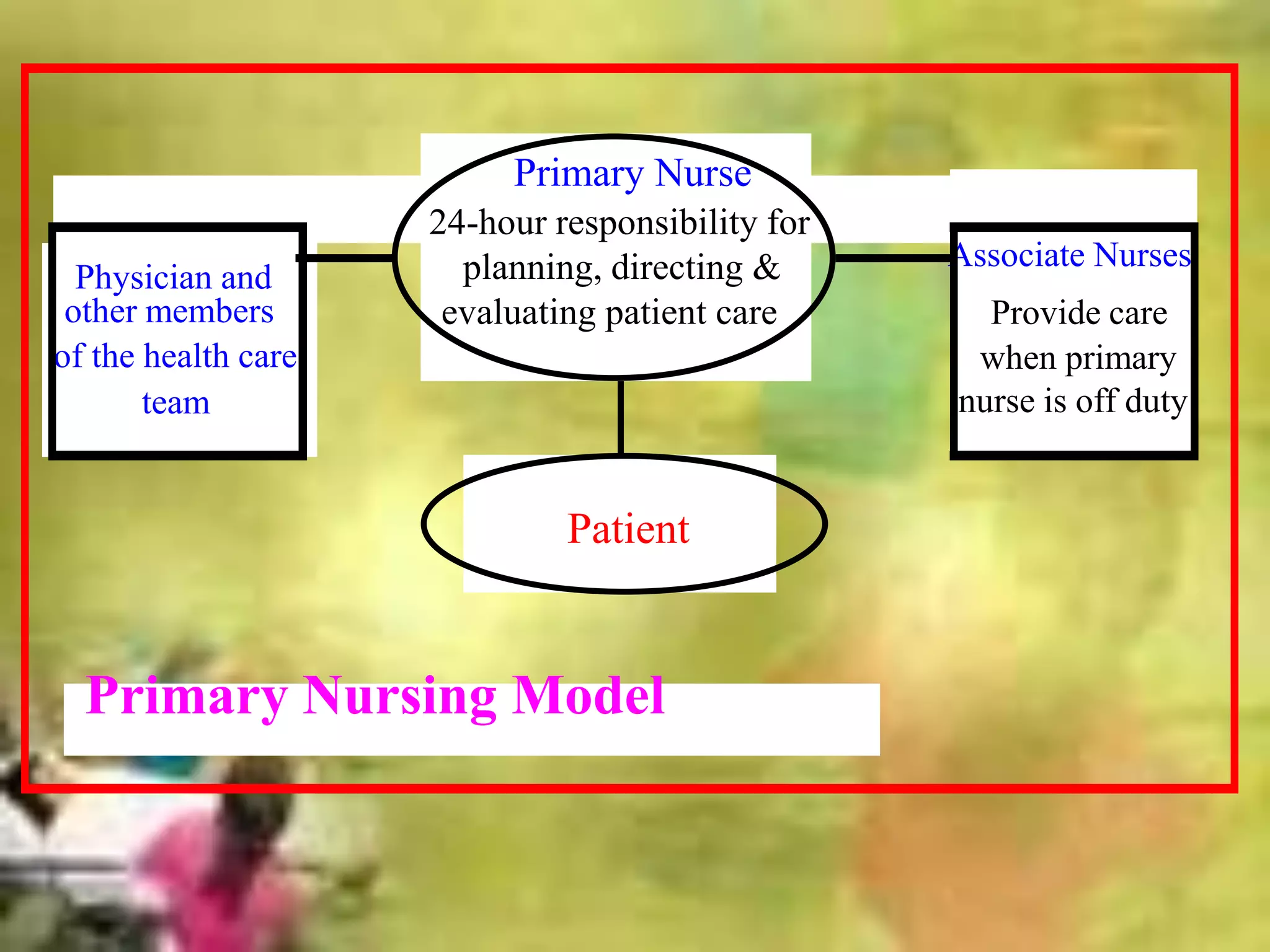
Primary Nurse
24-hour responsibilityfor
planning, directing &
evaluating patient care
Patient
Associate Nurses
Provide care
when primary
nurse is off duty
Physician and
other members
of the health care
team
Primary Nursing Model
47.
Merits:
opportunity forthe nurse to see the client and family as one
system.
Nursing accountability, responsibility and independence are
increased.
The nurse is able to use wide range of skills, knowledge and
expertise.
potentiates creativity by the nurse and thereby work
satisfaction increases
increased trust and satisfaction for both
48.
Demerits:
The nurse maybe isolated from the
colleagues.
Little avenue for group planning of care.
Nurse must be mature and independently
competent.
It must be cost effective.
49.
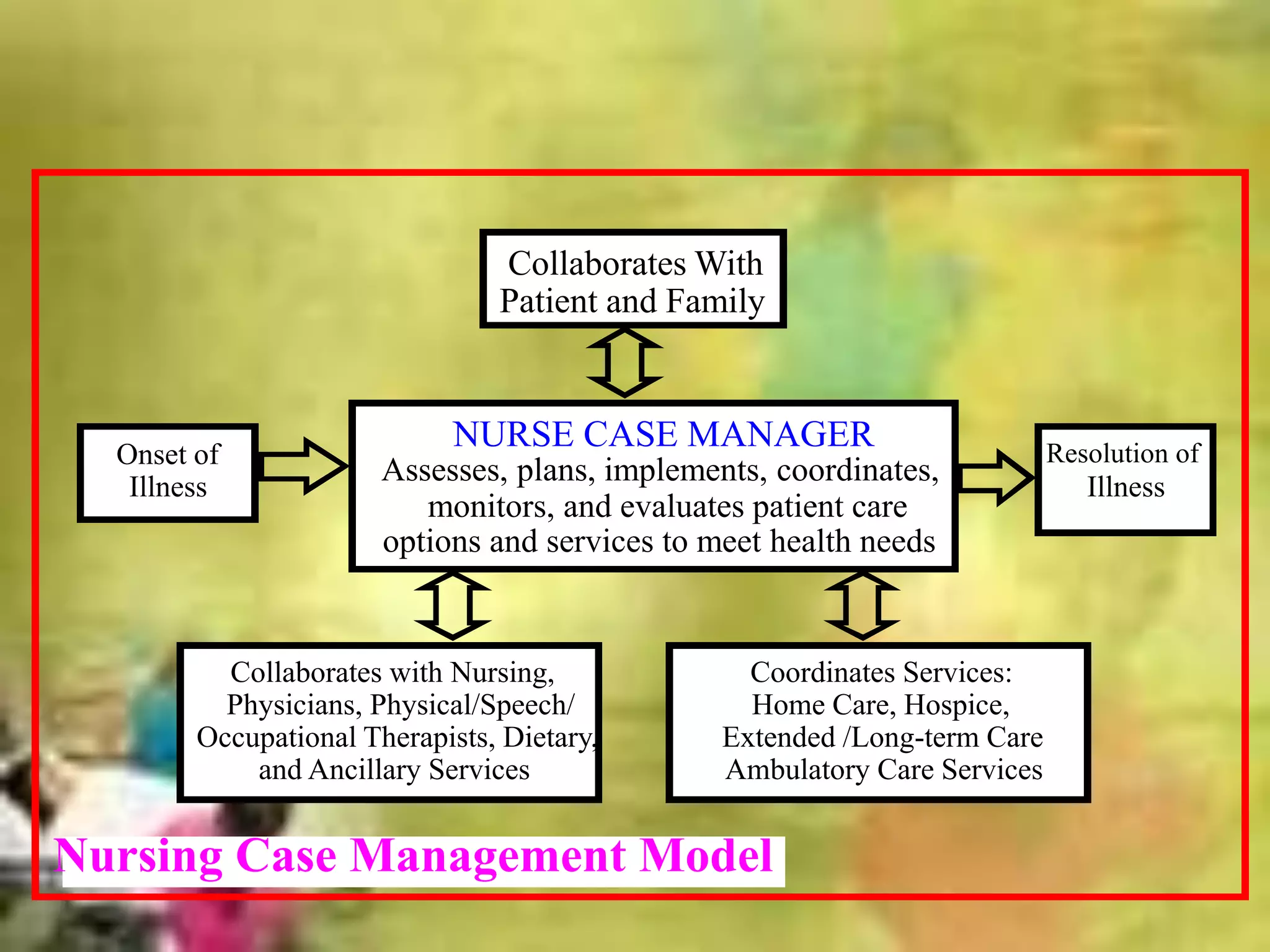
NURSE CASE MANAGER
Assesses,plans, implements, coordinates,
monitors, and evaluates patient care
options and services to meet health needs
Onset of
Illness
Resolution of
Illness
Collaborates with Nursing,
Physicians, Physical/Speech/
Occupational Therapists, Dietary,
and Ancillary Services
Collaborates With
Patient and Family
Coordinates Services:
Home Care, Hospice,
Extended /Long-term Care
Ambulatory Care Services
Nursing Case Management Model
50.
CASE MANAGEMENT MODEL
•Case management is a process of monitoring an
individual patient’s health care by the case manger,
for the purpose of maximizing positive outcomes
and containing costs. The case manger has
graduate-level preparation or is at an advanced
level of nursing practice. The case manager role
requires not only advanced nursing skills but also
advanced managerial and communication skills.
Advantages:
For the patient:-
• Establishing and achieving a set of “expected” or
standardized patient care outcomes for each patient.
• Facilitating early patient discharge or discharge within
an appropriate length of stay.
• Using the fewest possible appropriate health care
resources to meet expected patient care outcomes.
• Facilitating the continuity of patient care through
collaborative practice of diverse health professionals.
For the nurse: -
• Enhancing nurse’s professional development and job
satisfaction.
• Facilitating the transfer of knowledge of expert
clinical staff of novice staff.
55.
Disadvantages:
• Some expertsare argued that this role should be
reserved for the advance practitioner nurse or an
RN with advanced training or need 3 to 5 year
experience.
• The case manger should also be extremely bright,
have well developed interpersonal skills, be able
to multitask, have a strong foundation in
utilization review, and understand payer-patient
specifics and hospital reimbursement
mechanisms.
56.
DIFFERNTIATED NURSING PRACTICE
•Differentiated nursing practice refers to an
attempt to separate nursing practice roles based
on education or experience or some
combination of both.
57.
• Education model:
Roledifferentiation based upon type of
educational preparation [BSN, MSN etc]
• Competency model:
Role differentiation based on individual
nursing skills, expertise, experience etc.
58.
Merits:
• match patientsneeds with nursing
competencies.
• efficient use of nursing resources.
• Provide equitable compensation
• It increase nurse satisfaction, built loyalty
and increase the prestige of the nursing
profession.
59.
a prominent characteristicamong the new models
being tried is the nurse as a clinical expert
leading other members of the team partners.
60.
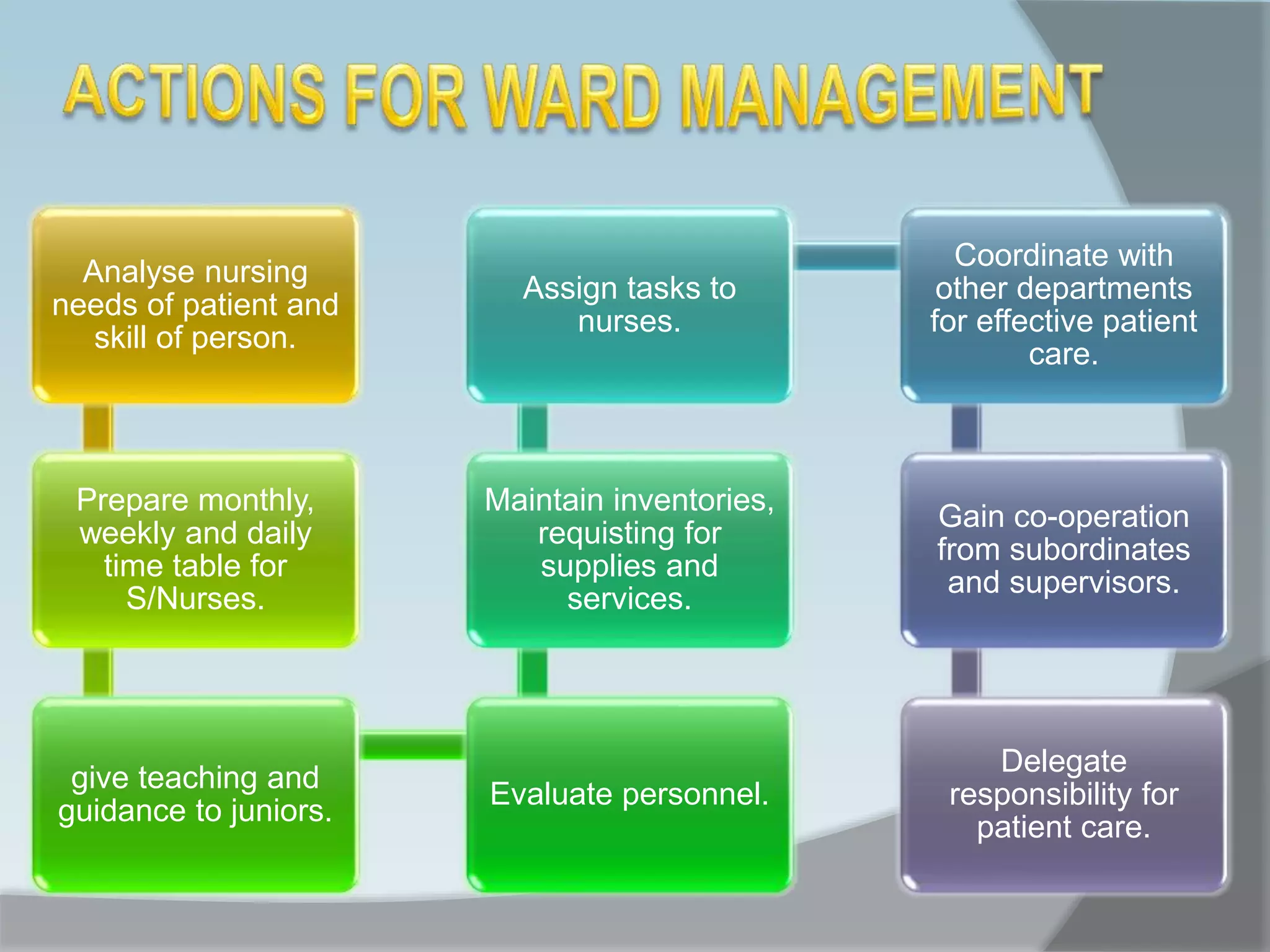
Analyse nursing
needs ofpatient and
skill of person.
Prepare monthly,
weekly and daily
time table for
S/Nurses.
give teaching and
guidance to juniors.
Evaluate personnel.
Maintain inventories,
requisting for
supplies and
services.
Assign tasks to
nurses.
Coordinate with
other departments
for effective patient
care.
Gain co-operation
from subordinates
and supervisors.
Delegate
responsibility for
patient care.
61.
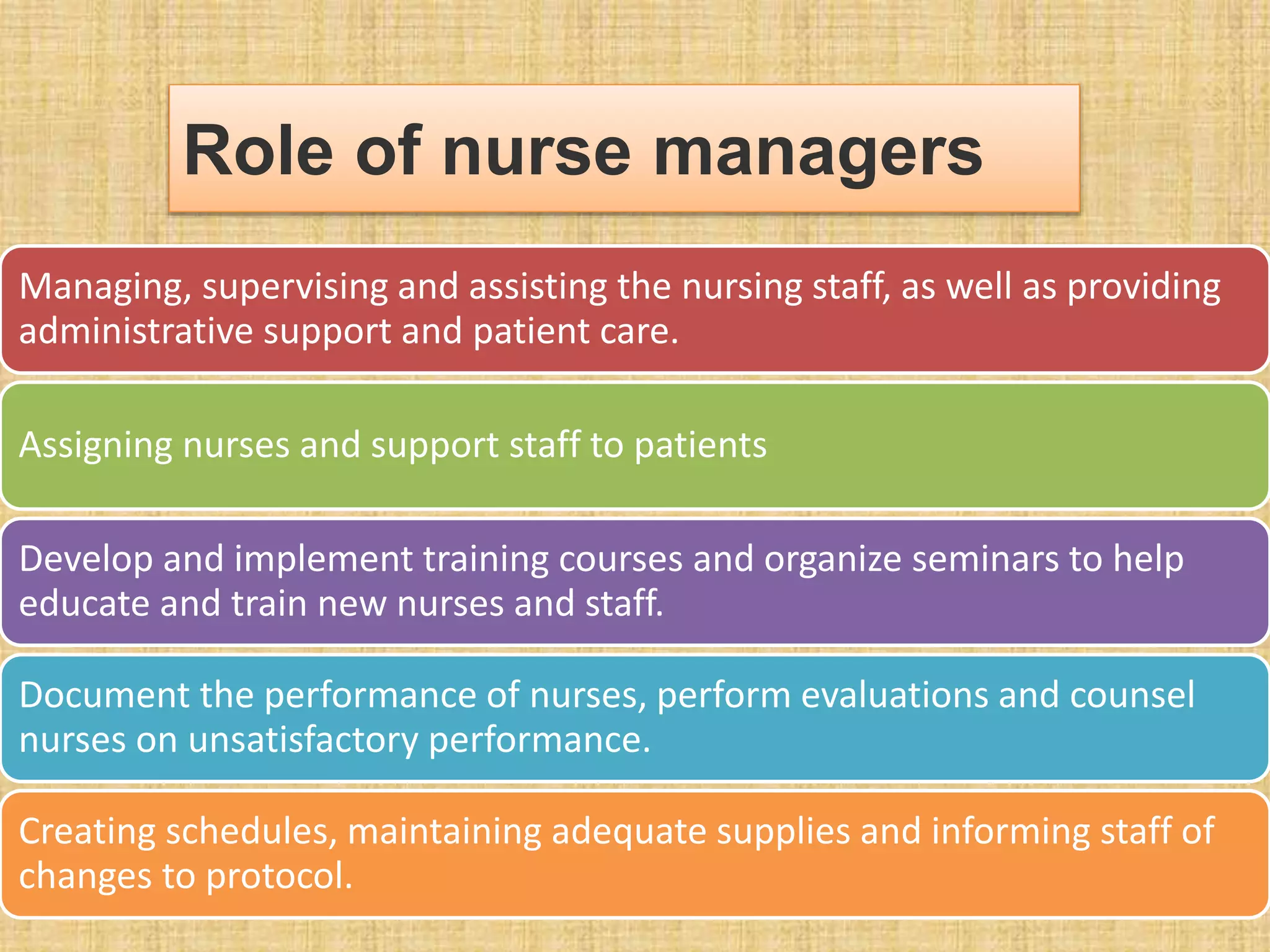
Managing, supervising andassisting the nursing staff, as well as providing
administrative support and patient care.
Assigning nurses and support staff to patients
Develop and implement training courses and organize seminars to help
educate and train new nurses and staff.
Document the performance of nurses, perform evaluations and counsel
nurses on unsatisfactory performance.
Creating schedules, maintaining adequate supplies and informing staff of
changes to protocol.
Role of nurse managers
62.
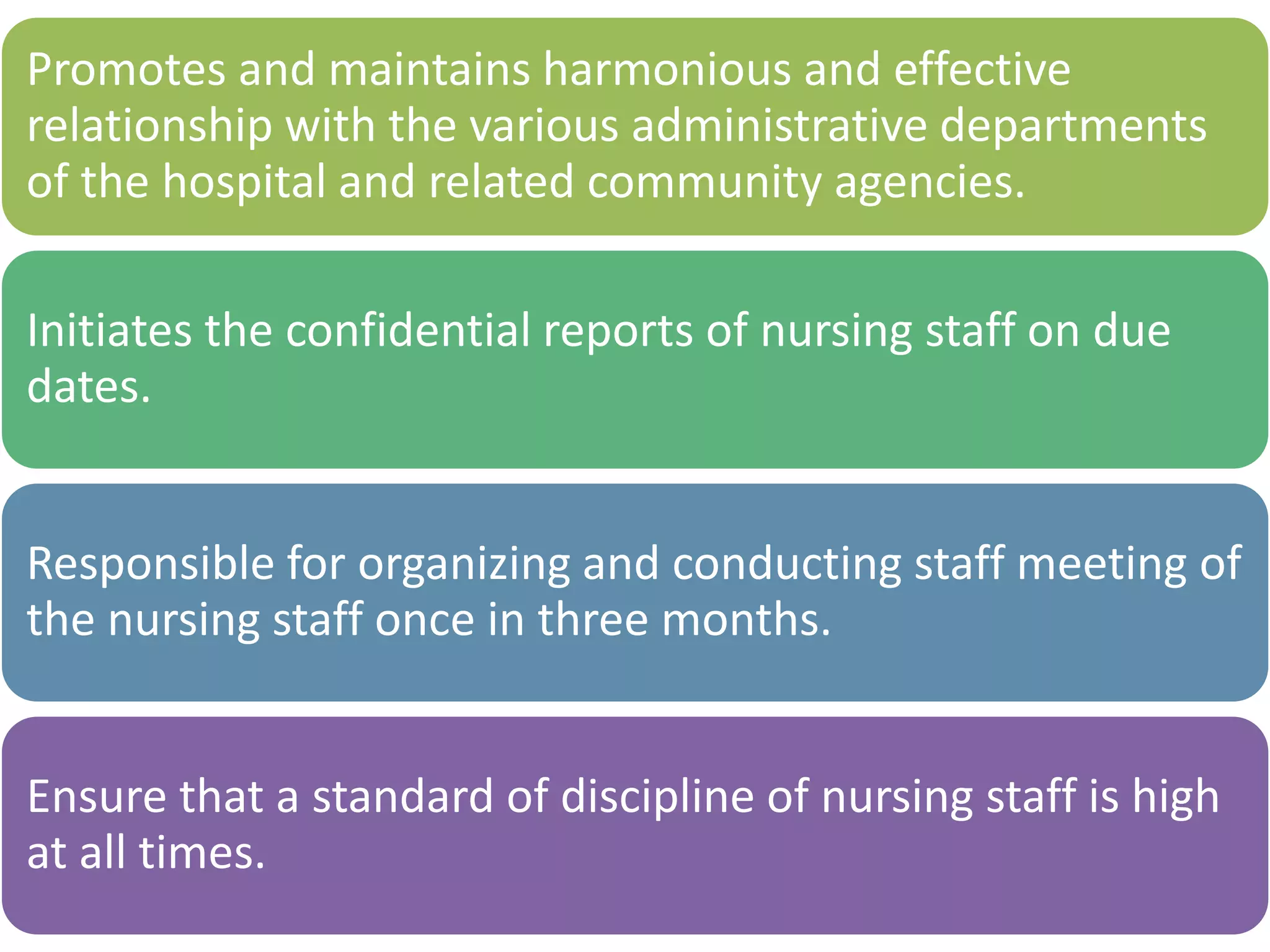
Promotes and maintainsharmonious and effective
relationship with the various administrative departments
of the hospital and related community agencies.
Initiates the confidential reports of nursing staff on due
dates.
Responsible for organizing and conducting staff meeting of
the nursing staff once in three months.
Ensure that a standard of discipline of nursing staff is high
at all times.
63.
Lack of adequate
training
Problemof
personnel
management
Inadequate
number of
nursing
staff
Shortage of
trained
manpower
No involvement
in planning.
No autonomy
in nursing
activities.
PROBLEMS AND CHALLENGES
64.
RESEARCH ARTICLES-:
1.The nurse-patientassignment: Purposes, decision factors and steps of the
process by Allen, Stephanie Brodack, Ph.D., UNIVERSITY OF SOUTH
CAROLINA, 2012,
The purpose of this exploratory descriptive study was to describe the nurse-
patient assignment process. Specifically, this study sought to identify
purposes, decision factors and steps of the process. Fourteen Nurse
Managers representing 11 nursing units of a suburban hospital in the
Southeastern United States were interviewed using a semi-structured
interview guide. The data was analyzed using Krippendorff's method of
content analysis. Results were presented in narrative and Venn diagram
form. The most common decision factors associated with the nurse-patient
assignment process were related to patient and nurse demographics, acuity,
proximity, competence, workload, nurse-patient ratio, collegiality and
staffing. Three pathways to making nurse-patient assignments were
described that corresponded to the type of nursing unit (episodic care, acute
care/short stay and long stay) on which they worked. For example, Nurse
managers on long stay units divided patients into groups then assigned the
nurse to a group of patients. Secondary findings indicated that nurse-patient
assignment process variations existed across the three unit types related to
purposes, decision factors, and steps of the nurse-patient assignment. For
example, the purposes discharge planning and care coordination were
identified only by Nurse Managers on long stay units.
65.
2. The Associationof Registered Nurse Staffing Levels and Patient
Outcomes: Systematic Review and Meta-Analysis
Kane, Robert L. MD et al Medical Care:December 2007 - Volume 45 - Issue
12 - pp 1195-1204 conducted a studyTo examine the association between
registered nurse (RN) staffing and patient outcomes in acute care
hospitals. . An increase by 1 RN per patient day was associated with a decreased
odds ratio of hospital acquired pneumonia (OR, 0.70; 95% CI, 0.56–0.88), unplanned
extubation (OR, 0.49; 95% CI, 0.36–0.67), respiratory failure (OR, 0.40; 95% CI, 0.27–
0.59), and cardiac arrest (OR, 0.72; 95% CI, 0.62–0.84) in ICUs, with a lower risk of
failure to rescue (OR, 0.84; 95% CI, 0.79–0.90) in surgical patients. Length of stay was
shorter by 24% in ICUs (OR, 0.76; 95% CI, 0.62–0.94) and by 31% in surgical patients
(OR, 0.69; 95% CI, 0.55–0.86).
Studies with different design show associations between increased RN staffing and
lower odds of hospital related mortality and adverse patient events. Patient and
hospital characteristics, including hospitals’ commitment to quality of medical care,
likely contribute to the actual causal pathway.
66.
Yu-Chih Chen etal (2013) did a quasi experimental study on Effectiveness of
nurse case management compared with usual care in cancer patients at a
single medical center in Taiwan:
This study was conducted with a quasi-experimental design in a national
medical center in Northern Taiwan. A total number of 600 subjects randomly
selected from the cancer case management system enrolled in the case
managed group, and 600 patients who received usual care were randomly
selected from cancer registry and enrolled in the control group. The study
instrument was developed to measure care effectiveness, including the rates of
patient continuing treatment, non-adherence to treatment, prolonged
hospitalization, unplanned readmission, and planned admission for active
treatment.
Researcher concluded that cancer case management could improve the
effectiveness of cancer care services and concretely illustrated a
comprehensive model for oncology patients in Taiwan and suggested for further
investigation.
Instruct the staff
nurseto stay on
patients left side
to help in
patient’s
examination.
Remember and
report
observation to
doctor.
record orders/get
them written by
doctors.
After the ward
Round:
• Instruct staff nurses
to carry out orders
• Observe patient
carefully.






![• Education model:
Role differentiation based upon type of
educational preparation [BSN, MSN etc]
• Competency model:
Role differentiation based on individual
nursing skills, expertise, experience etc.](https://image.slidesharecdn.com/pptformgmt-161210080235/75/methods-os-patient-assignment-57-2048.jpg)