Downloaded 16 times









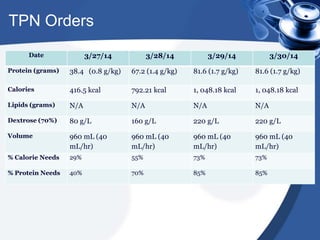








This document provides details about a 40-year-old female patient who presented with malnutrition due to chronic alcoholic pancreatitis, liver cirrhosis, and a history of gastric bypass surgery performed 10 years prior. She was admitted to the hospital for placement of a PICC line and initiation of total parenteral nutrition (TPN) due to failure to thrive. Her hospital course and treatment are described, including monitoring of her nutritional status and prescription of TPN to meet her nutrient needs. The case highlights the importance of thorough nutritional assessment and management of patients with complex medical histories and nutritional complications following bariatric surgery.












































































