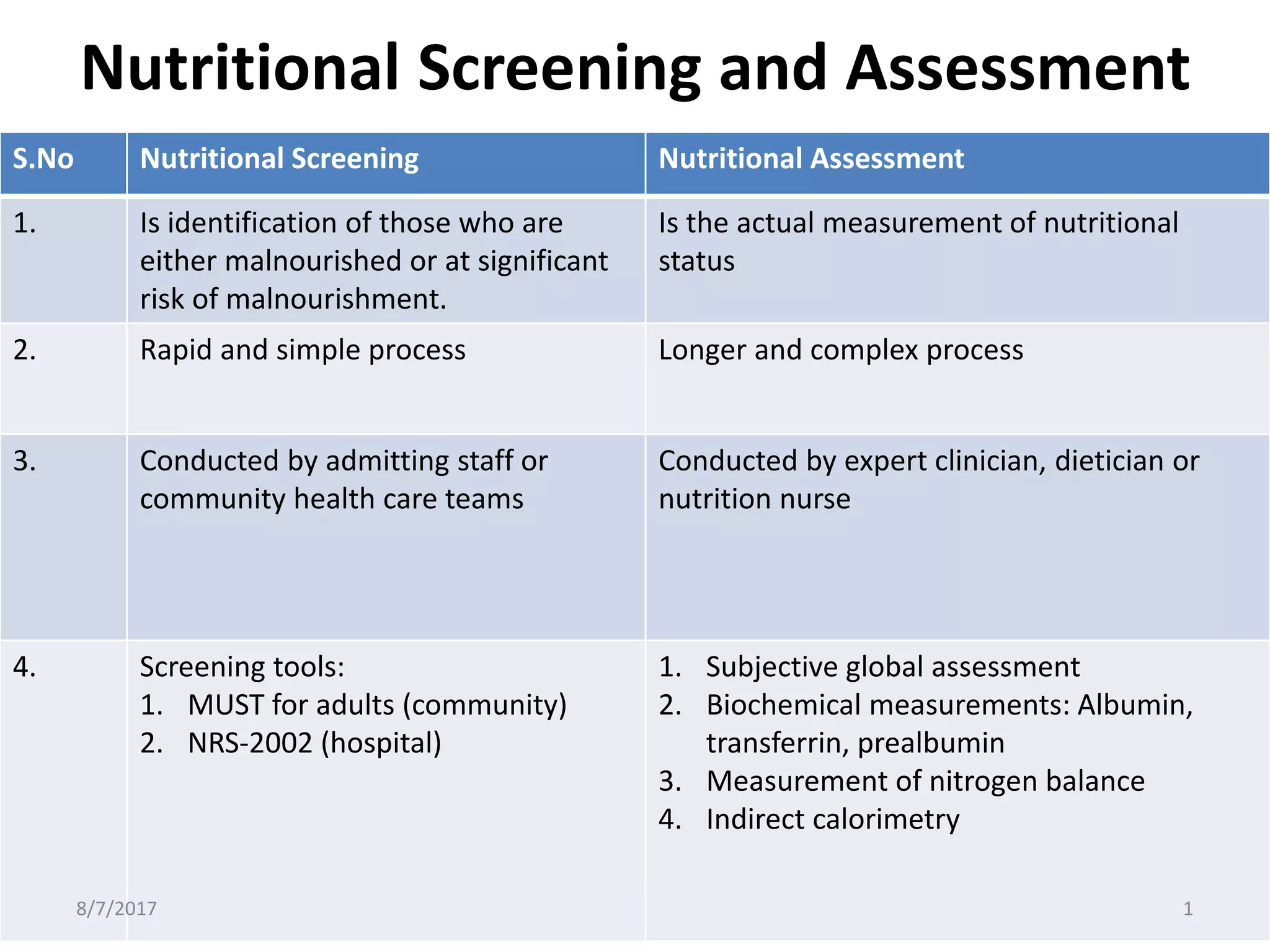
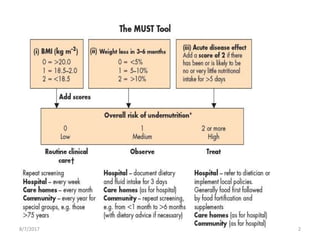
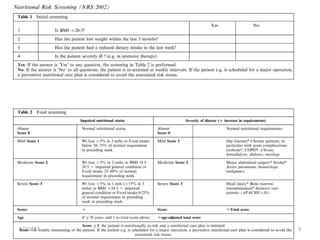
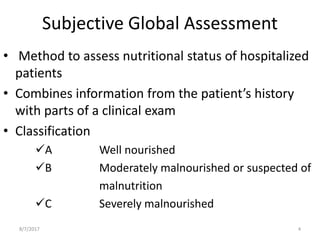
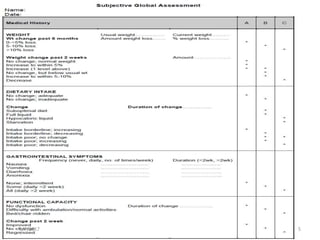
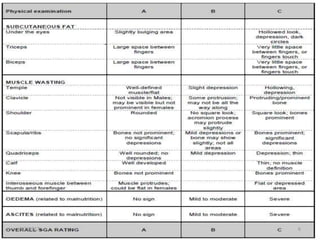
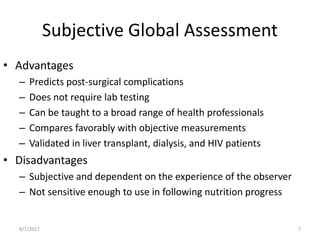
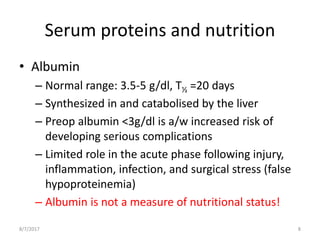
Nutritional screening and assessment involve identifying at-risk individuals and measuring nutritional status. Screening uses simple tools to rapidly identify malnutrition risk, while assessment uses more complex clinical and laboratory tests conducted by experts. Key assessment methods include subjective global assessment of history and exam, laboratory markers like albumin and prealbumin, and objective tests such as indirect calorimetry and nitrogen balance measurements. Assessment helps predict patient outcomes and nutritional requirements.