Downloaded 42 times

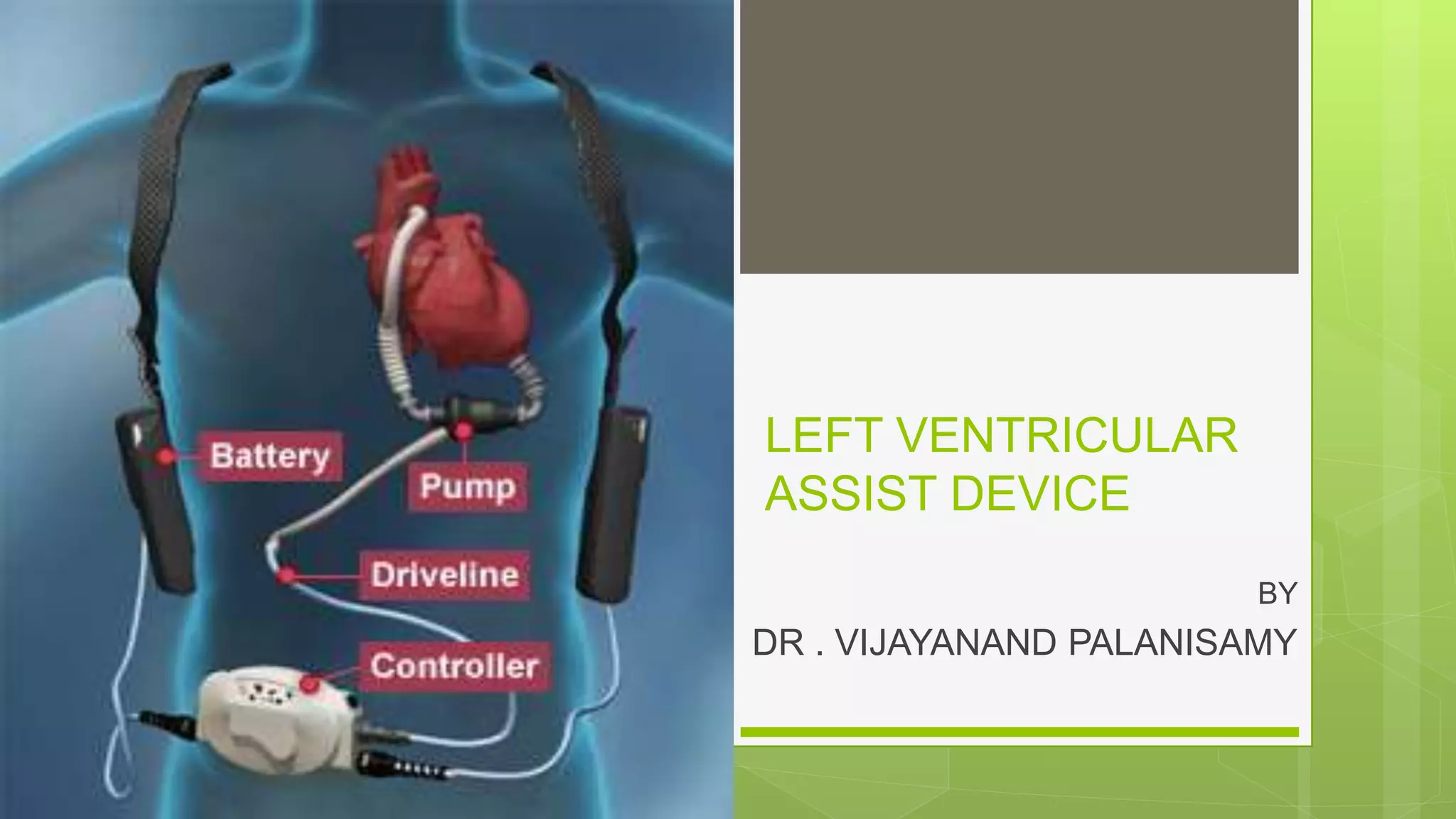
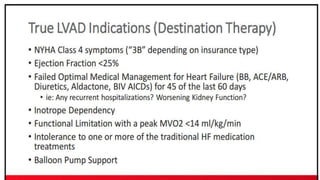
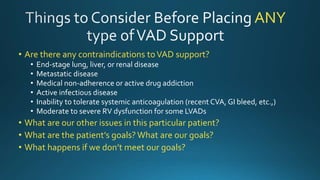
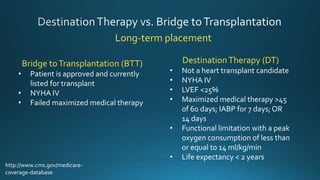
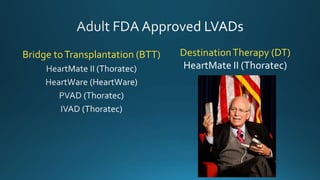
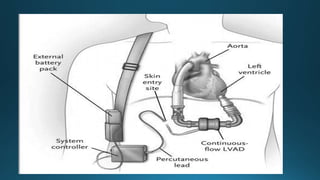
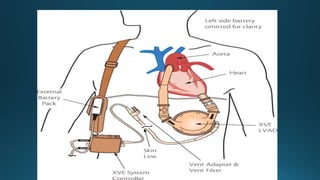
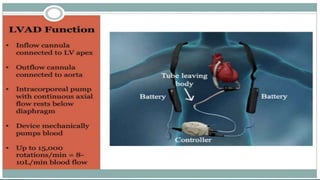
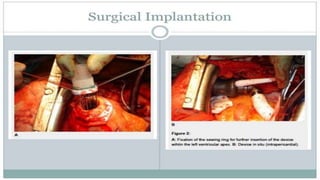
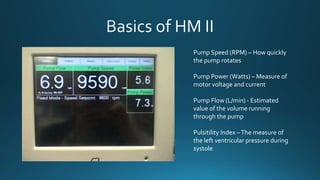
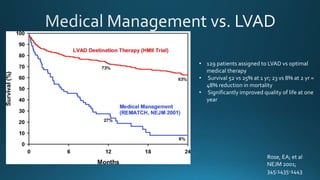
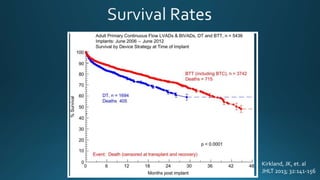
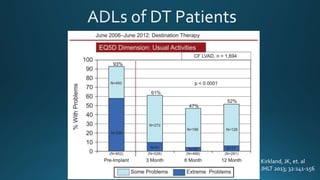
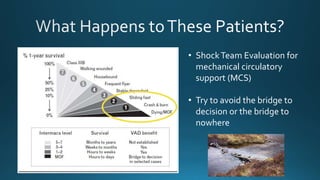

This document discusses left ventricular assist devices (LVADs) including: - Types of LVAD support including bridge to transplantation, destination therapy, and devices like the HeartMate II. - Contraindications and patient criteria for LVAD support. - Components and functions of the LVAD including the external controller. - Monitoring of pump parameters on the controller. - Potential complications of LVAD support. - Clinical trial results demonstrating improved survival and quality of life with LVADs.






































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













