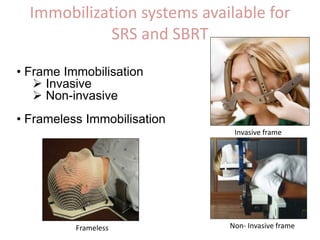
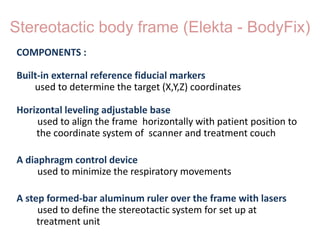
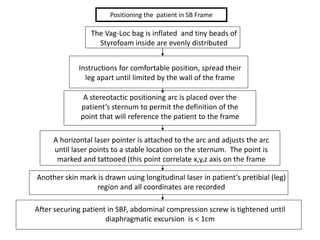
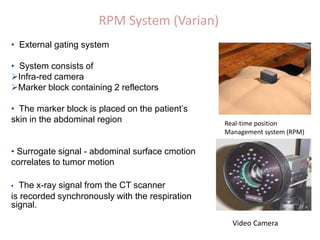
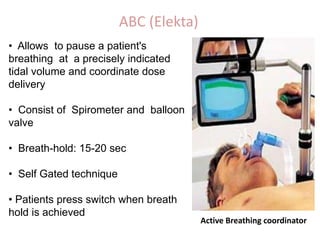
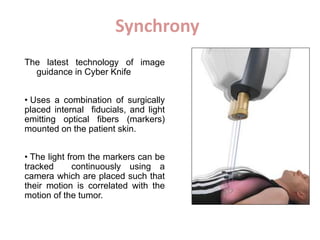
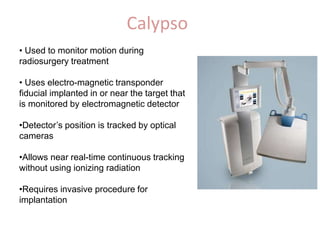
Immobilization and positioning techniques are essential for accuracy in stereotactic radiosurgery (SRS) and stereotactic body radiotherapy (SBRT). There are invasive and non-invasive immobilization systems for the head and body that use customized masks, frames, or bite blocks. Repositioning is aided by various fiducial marker systems. Motion management techniques include gating using the active breathing coordinator or respiratory position management systems. Emerging real-time tumor tracking methods allow for continuous beam adjustment to target motion during treatment. Precise immobilization and motion management are needed to minimize positioning errors and ensure accurate dose delivery in SRS and SBRT.