This document discusses vascular trauma to the lower limbs, specifically:
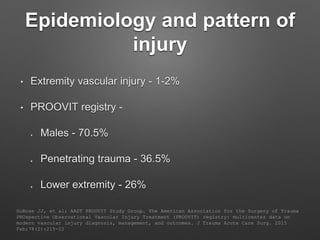
1. It provides epidemiological data on lower limb vascular injuries, noting they make up 26% of extremity injuries and are more common in males from penetrating trauma.
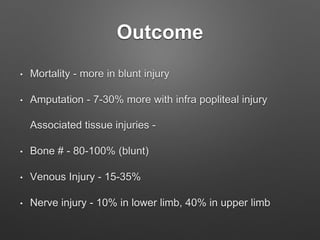
2. Outcomes include higher mortality rates for blunt injuries and amputation rates ranging from 7-30% for injuries below the knee. Associated bone fractures occur in 80-100% of blunt injuries.
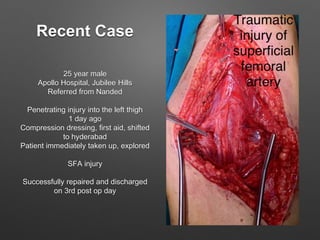
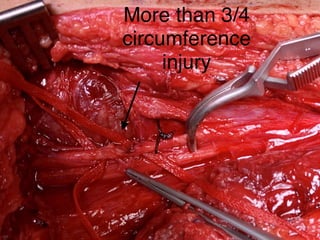
3. Examination findings and investigations like Doppler, CT angiography are discussed for evaluating the extent of injury.
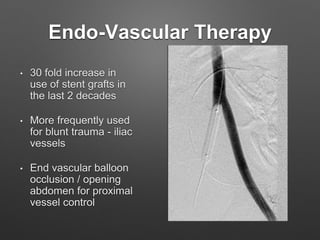
4. Treatment principles covered include non-operative management for small injuries, endovascular techniques for iliac vessels, and open surgical repair with grafts and








































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






