Download to read offline

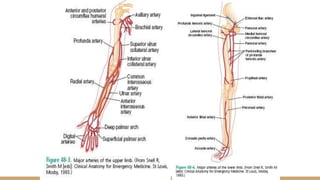
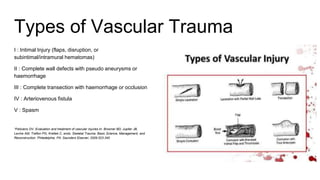
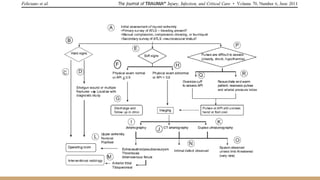
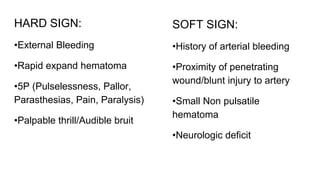
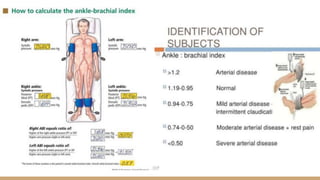
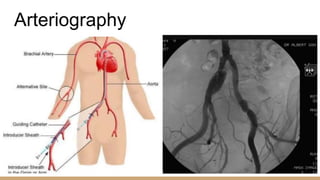

This document summarizes the history and classification of peripheral vascular injuries. It discusses that peripheral vascular injuries most commonly involve the extremities, with 50-60% occurring in the femoral/popliteal region and 30% in the brachial region. The causes are typically penetrating trauma like gunshots or stab wounds (80%) or blunt trauma. Vascular injuries are classified into 5 types ranging from intimal injuries to complete transections. Physical exam signs of vascular injury can include external bleeding, expanding hematoma, pulselessness, pallor, parasthesias, pain, paralysis, or palpable thrills/audible bruits. Arteriography is important for diagnosis, as timeliness is crucial to avoid life-




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













