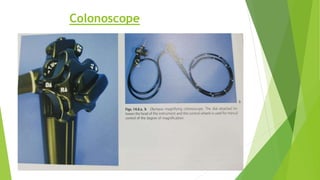
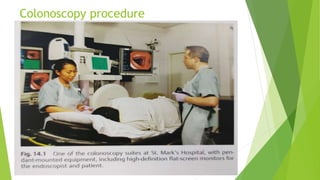
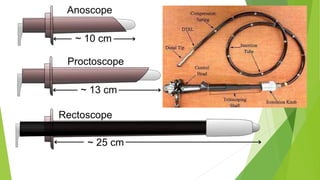
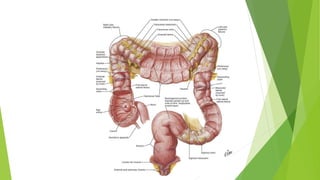
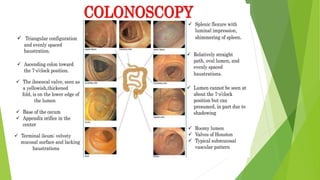
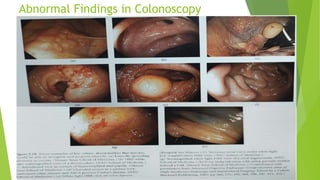
Lower GI endoscopy procedures like colonoscopy and sigmoidoscopy allow examination of the interior of the large intestine. Colonoscopy uses a flexible tube 110-140cm long to view the entire colon, and is helpful for evaluating changes in bowel habits, bleeding, and screening for colorectal cancer. It requires bowel preparation with clear liquids and laxatives. Sigmoidoscopy can examine the descending colon and rectum using a rigid or flexible short tube. Both procedures provide direct visualization of the intestinal lining and any abnormalities.