Downloaded 17 times
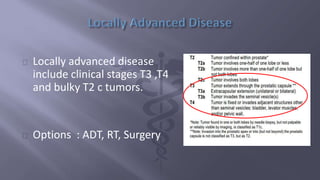
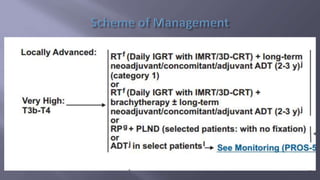
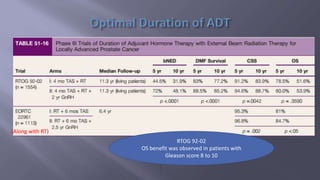
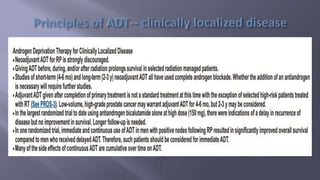
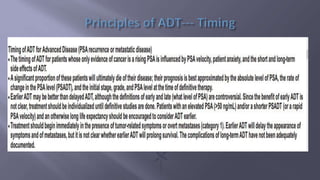
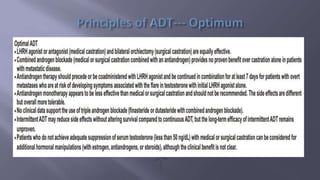
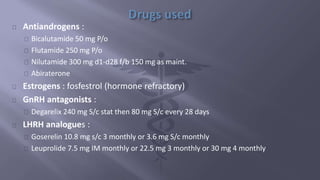


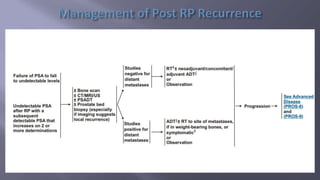

This document discusses treatment options for locally advanced prostate cancer, including androgen deprivation therapy (ADT), radiation therapy (RT), and surgery, highlighting the effectiveness and side effects of various combinations. It presents findings from multiple randomized trials emphasizing the importance of total androgen suppression and regional radiotherapy in improving tumor control and survival rates. Additionally, it provides guidelines for managing potential side effects such as cardiovascular events and bone mineral density loss during treatment.
































![Ca prostate [edmond]](https://cdn.slidesharecdn.com/ss_thumbnails/caprostateedmond-130318091345-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)