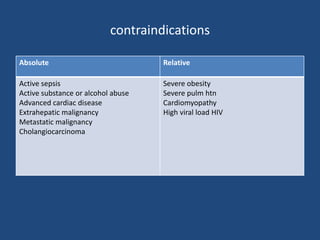
Liver transplantation involves surgically removing a diseased liver and replacing it with a healthy donor liver. It is the only cure for end-stage liver disease. The first successful human liver transplant was performed in 1967. Liver transplantation can treat conditions such as cirrhosis, hepatitis, cancer and genetic disorders. Potential donors can be deceased or living. Living donors allow for shorter wait times but carry surgical risks. Anesthesia involves careful management of hemodynamic, metabolic and coagulation abnormalities during the different surgical phases. Postoperative care focuses on monitoring liver function, preventing infections and managing complications.
![• The Model for End-stage Liver Disease (MELD) score is used
by the United Network for Organ Sharing (UNOS) to prioritize
patients on the waiting list for a liver transplant
• Th e MELD score = 0.957 × log e [serum creatinine
(mg/dL)] + 0.378 × log e [total serum bilirubin (mg/dL)]
+ 1.120 × log e [INR]
• A score of 20 predicts a 19.6% risk of mortality at 3 months,
whereas a score of 40 predicts a 71.3% risk of mortality at
3 months](https://image.slidesharecdn.com/livertransplantation-170228112508/85/Liver-transplantation-and-anaesthetic-management-10-320.jpg)





















































![sagana liver [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/saganaliverautosaved-231108132136-9fe68f5d-thumbnail.jpg?width=640&height=640&fit=bounds)





















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)