Downloaded 85 times







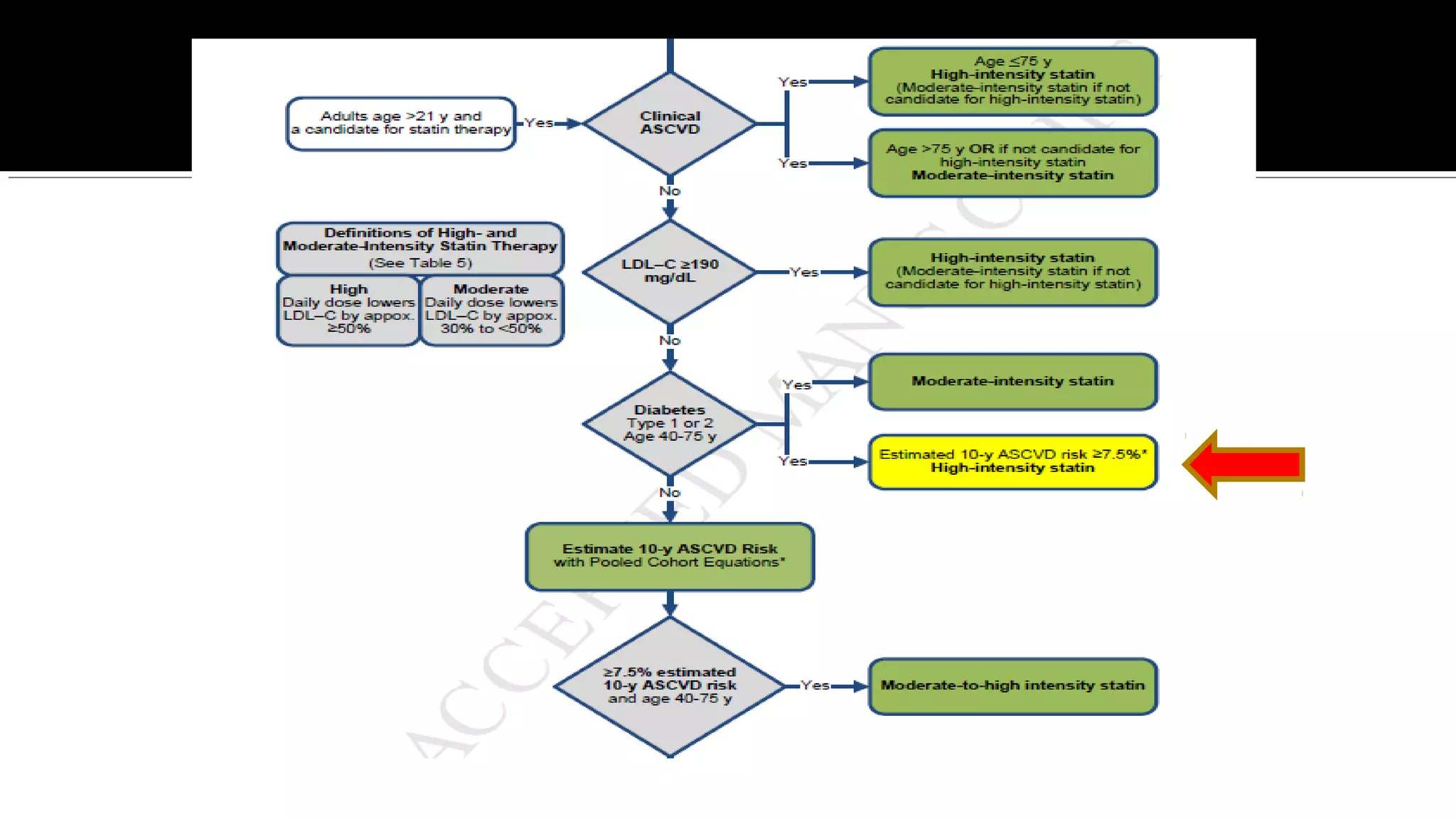
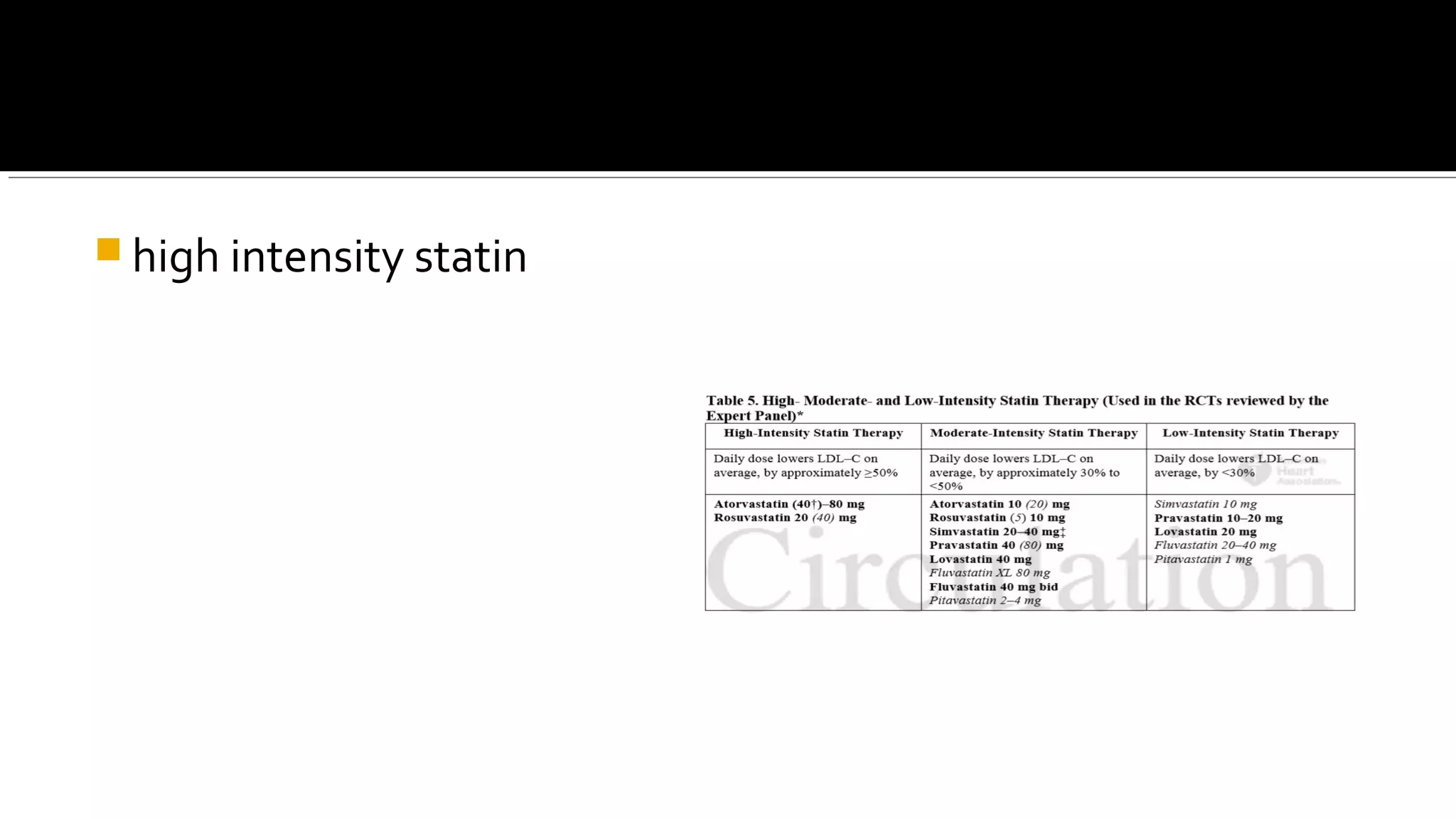
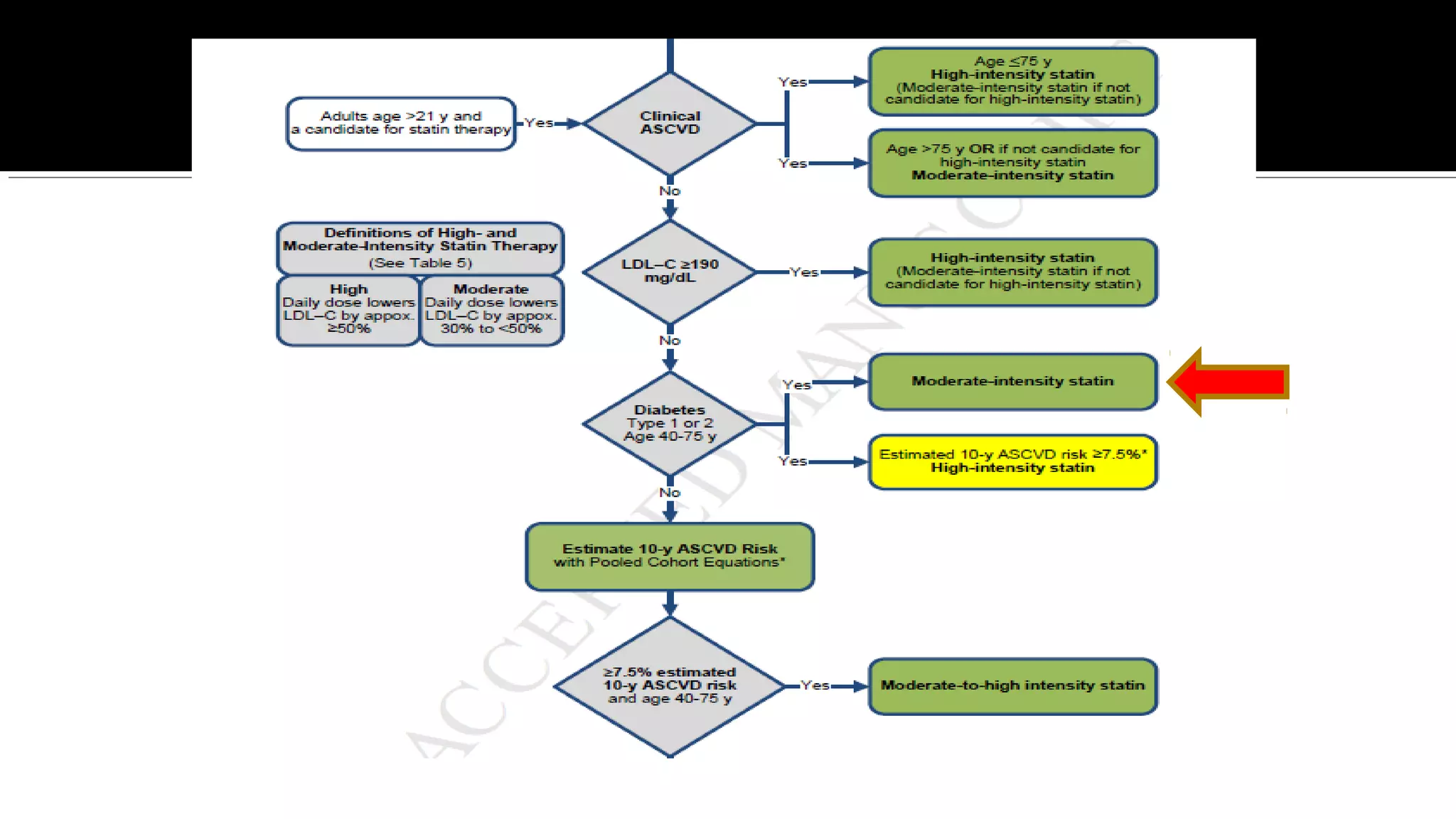
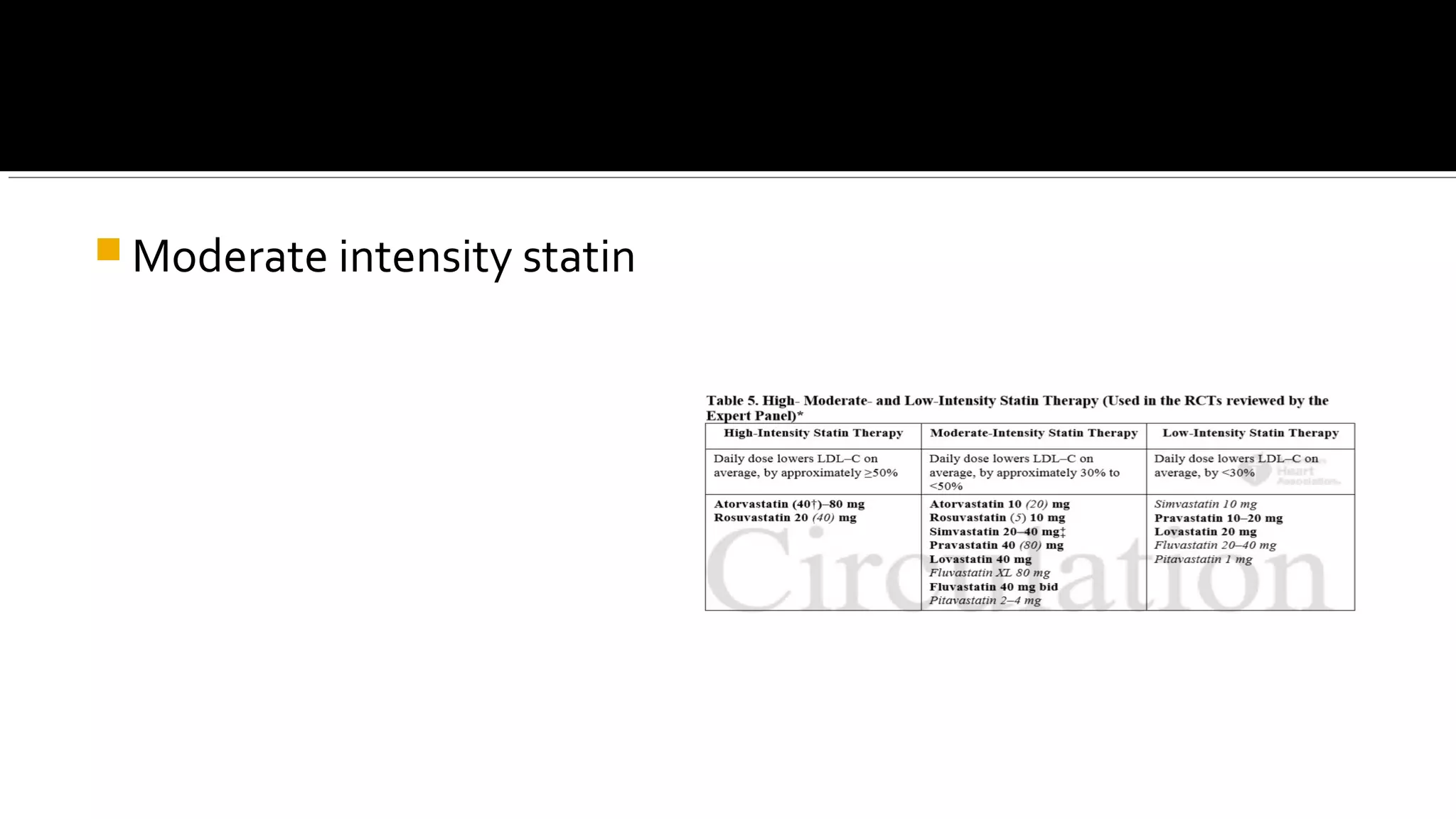








1. The new guidelines recommend initiating moderate or high-intensity statin therapy for patients in four categories based on their cardiovascular risk, rather than targeting a specific LDL-C level. 2. The four categories are: individuals with clinical atherosclerotic cardiovascular disease, LDL-C over 190 mg/dL, diabetes between ages 40-75 with LDL-C 70-189 mg/dL, and 10-year risk over 7.5% for ages 40-75 with LDL-C 70-189 mg/dL. 3. Lipids should be measured during follow-ups to assess adherence, not to achieve a specific target level.





































































































