Downloaded 71 times
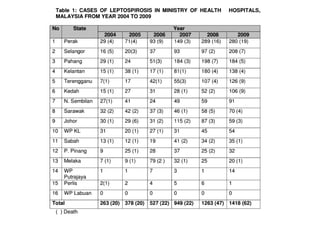
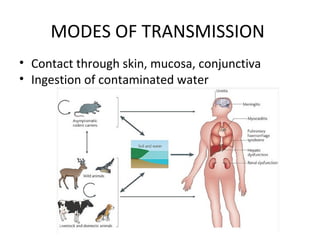
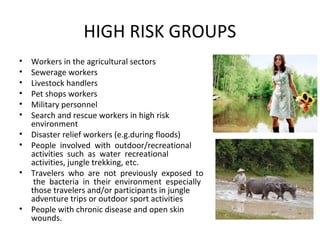
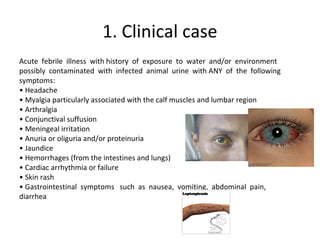

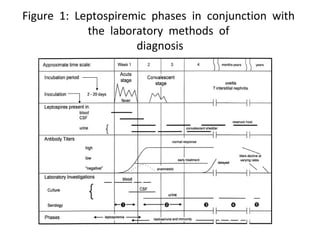
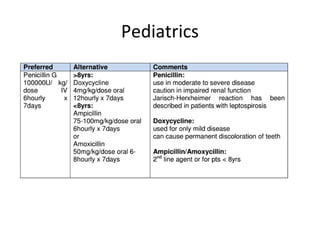
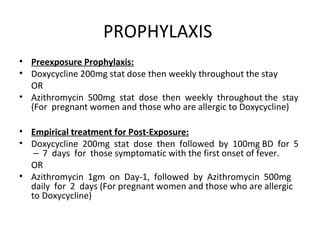
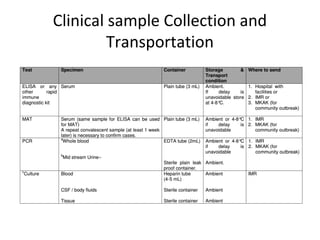


Leptospirosis is a zoonotic bacterial disease caused by Leptospira interrogans bacteria transmitted from infected animals to humans through contact with water or soil contaminated by animal urine. It has a wide range of clinical manifestations from a mild flu-like illness to potentially fatal Weil's disease affecting the liver and kidneys. High risk groups include agricultural, sewer and military workers exposed to contaminated environments. Diagnosis involves serological tests or culture of the bacteria from blood or urine, with treatment consisting of antibiotics like doxycycline or penicillin. Prevention focuses on minimizing exposure through protective equipment and chemoprophylaxis of high risk groups.






































![Hidup Sihat Bebas Kencing Manis Diabetes [eBook]](https://cdn.slidesharecdn.com/ss_thumbnails/ebook-hidupsihatbebaskencingmanis-170128182257-thumbnail.jpg?width=640&height=640&fit=bounds)