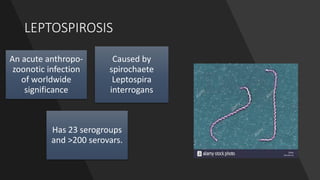
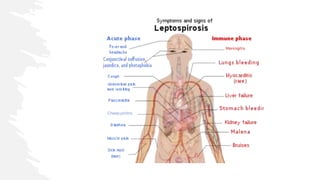
Leptospirosis is a bacterial infection caused by Leptospira interrogans bacteria. It is transmitted through contact with water or soil contaminated by the urine of infected animals like rats. Common symptoms include fever, muscle pain, jaundice, and potentially life-threatening organ damage. Treatment involves antibiotics like doxycycline or penicillin. Prevention strategies focus on education, personal protective measures for high risk groups like farmers, rodent control, vaccination of animals in endemic areas, and chemoprophylaxis with doxycycline during peak transmission seasons.