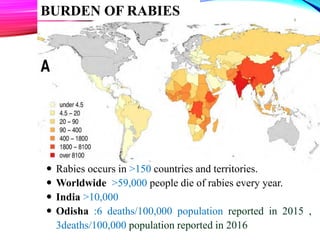
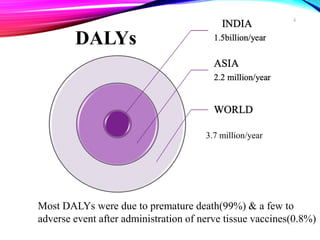
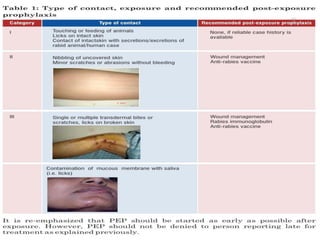
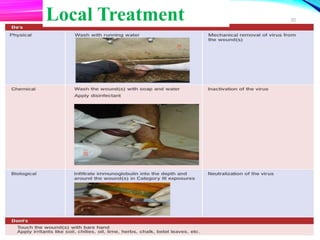
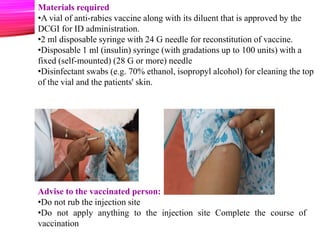
This document provides an overview of rabies, including its epidemiology, clinical manifestations, classification of animal bites, prevention, and control programs. Rabies is a fatal viral infection transmitted through animal bites that is preventable through vaccination. It remains a public health problem worldwide, with tens of thousands of deaths annually, primarily in Asia and Africa. Dogs are the main reservoir and source of human infections. Post-exposure prophylaxis including wound cleansing and vaccination is effective but must be administered promptly after exposure to prevent onset of symptoms.