Introduction,
Left Heart Catheterization,
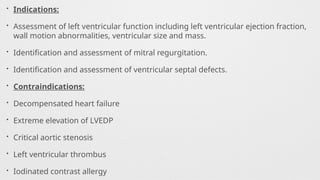
Indications,
Contraindications,
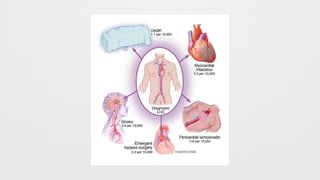
Complications,
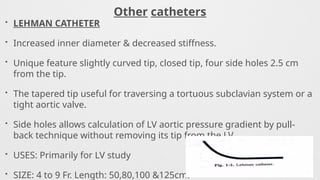
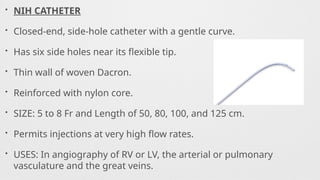
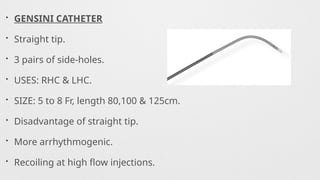
Catheters Used,
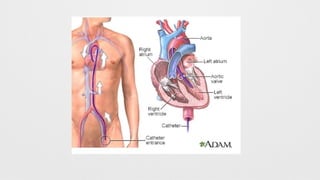
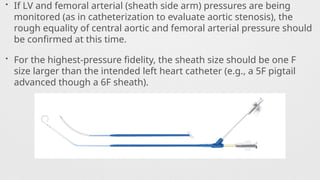
Procedure,
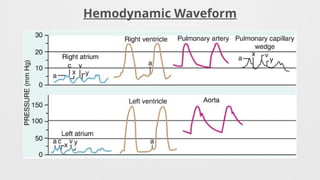
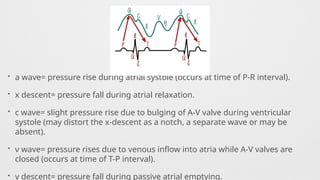
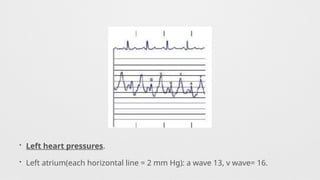
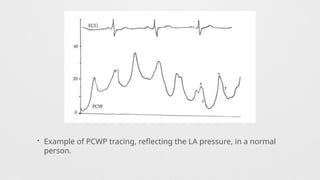
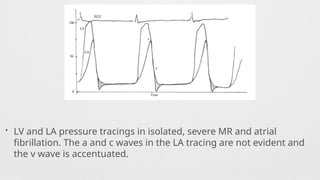
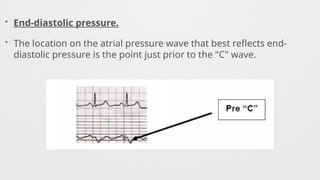
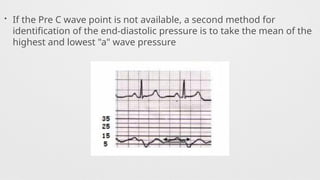
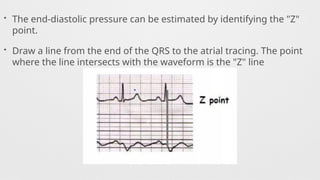
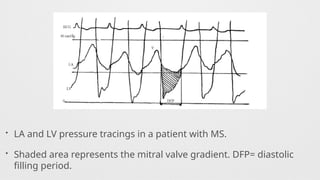
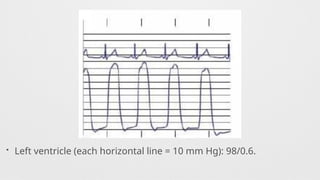
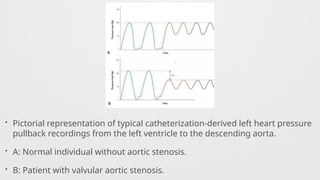
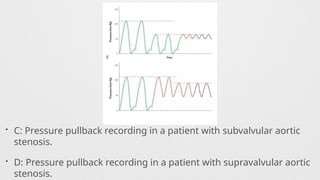
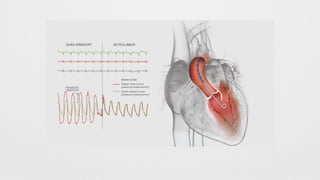
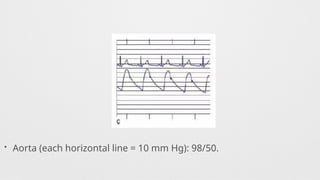
Hemodynamics,
Hemodynamics data,
Shunt Calculation,
Oxymetry,
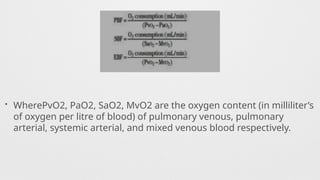
Shunt Quantification,
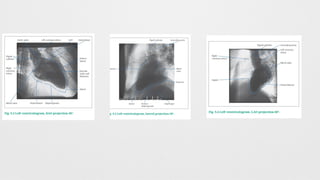
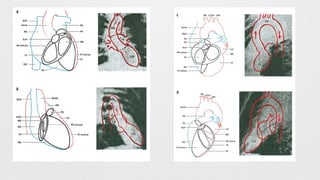
Left Ventriculogram,
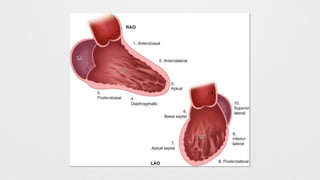
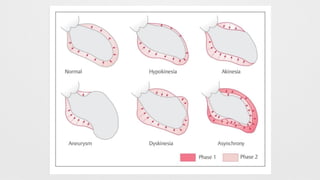
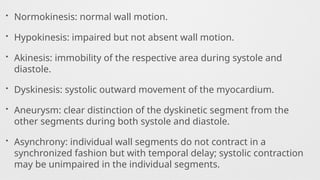
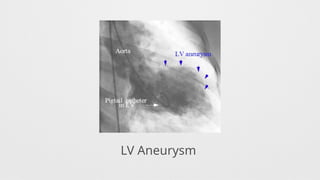
LV Wall motion abnormalities,
Angiographic Aortic Regurgitation,
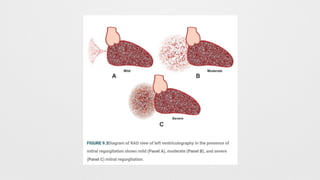
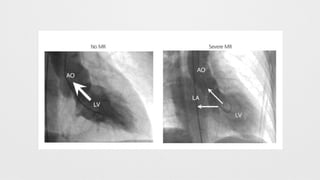
Angiographic Mitral Regurgitation


























![Invasive_Cardio-Devices_procedures[1].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/invasivecardio-devicesprocedures1-240129085722-eb86cfb0-thumbnail.jpg?width=640&height=640&fit=bounds)


























