Downloaded 35 times


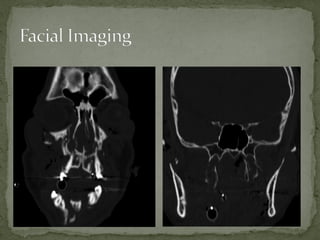

A 38-year-old man was found unconscious 40 yards from the scene of a motorcycle accident. He had obvious facial trauma including a midface fracture, severe facial edema, and blood in his oropharynx. His vital signs included a temperature of 98.6 F, heart rate of 120, respiratory rate of 12, and oxygen saturation of 90% on a nasal cannula with a blood pressure of 95/60. His Glasgow Coma Scale was 8. Imaging showed right type III and bilateral pterygoid fractures. He required intubation, ophthalmology consultation, and admission to the operating room for open reduction and internal fixation of his facial fractures.