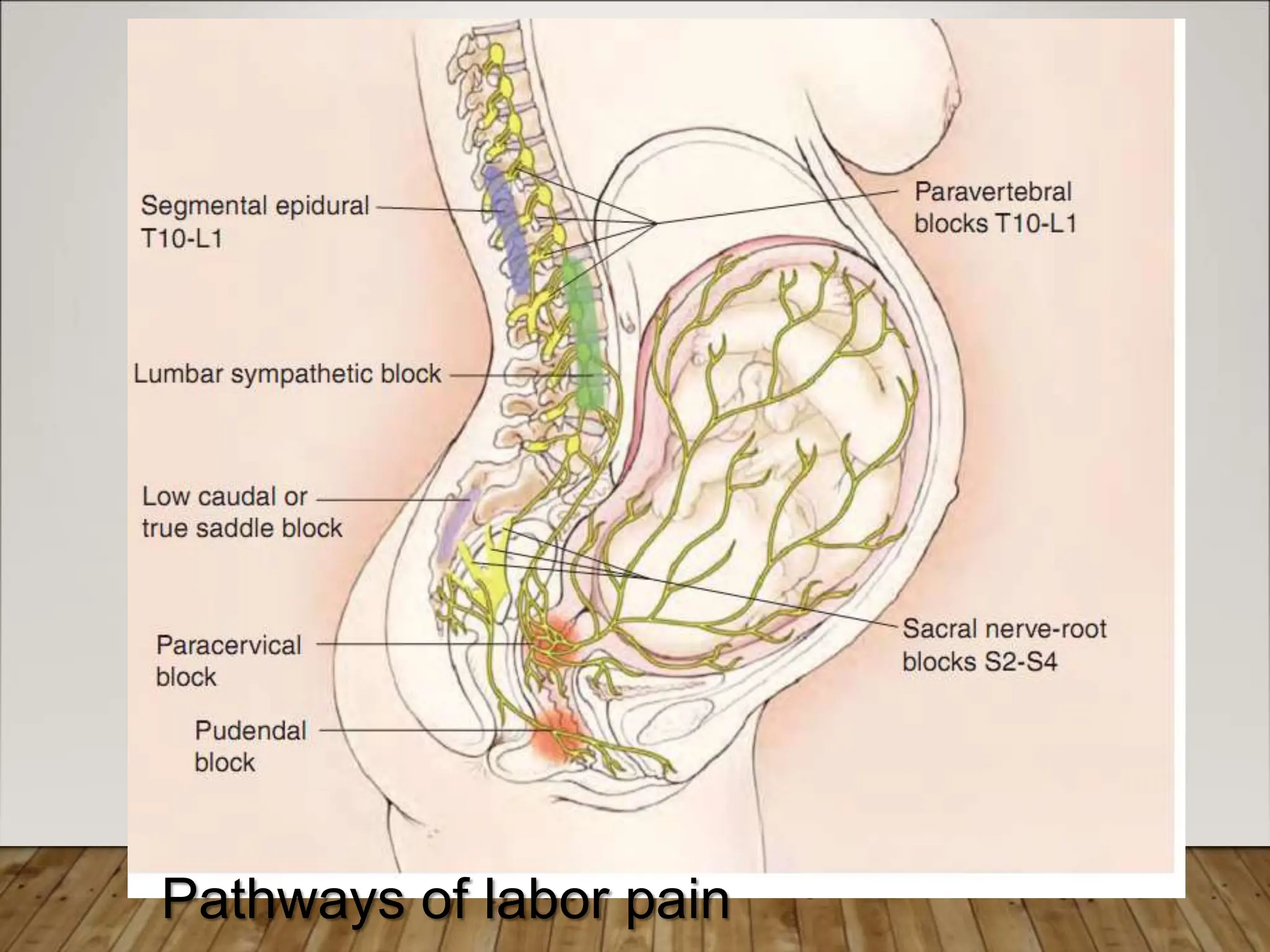
John Snow popularized the use of pain relief during labor by administering chloroform to Queen Victoria for the birth of her eighth child. Labor and delivery result in severe pain that is greater than a fractured arm or cancer pain. Only two conditions are more painful than labor. It is important to have an anesthesiologist dedicated to pain management during labor and delivery to safely provide pain relief options. Epidural analgesia provides the best pain relief for labor but other options like intravenous opioids, nitrous oxide, and regional nerve blocks are available depending on the specific situation.

































































![menstrual cycle [Autosaved]-2 (5).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/menstrualcycleautosaved-25-230321042311-7c0898c3-thumbnail.jpg?width=640&height=640&fit=bounds)






















