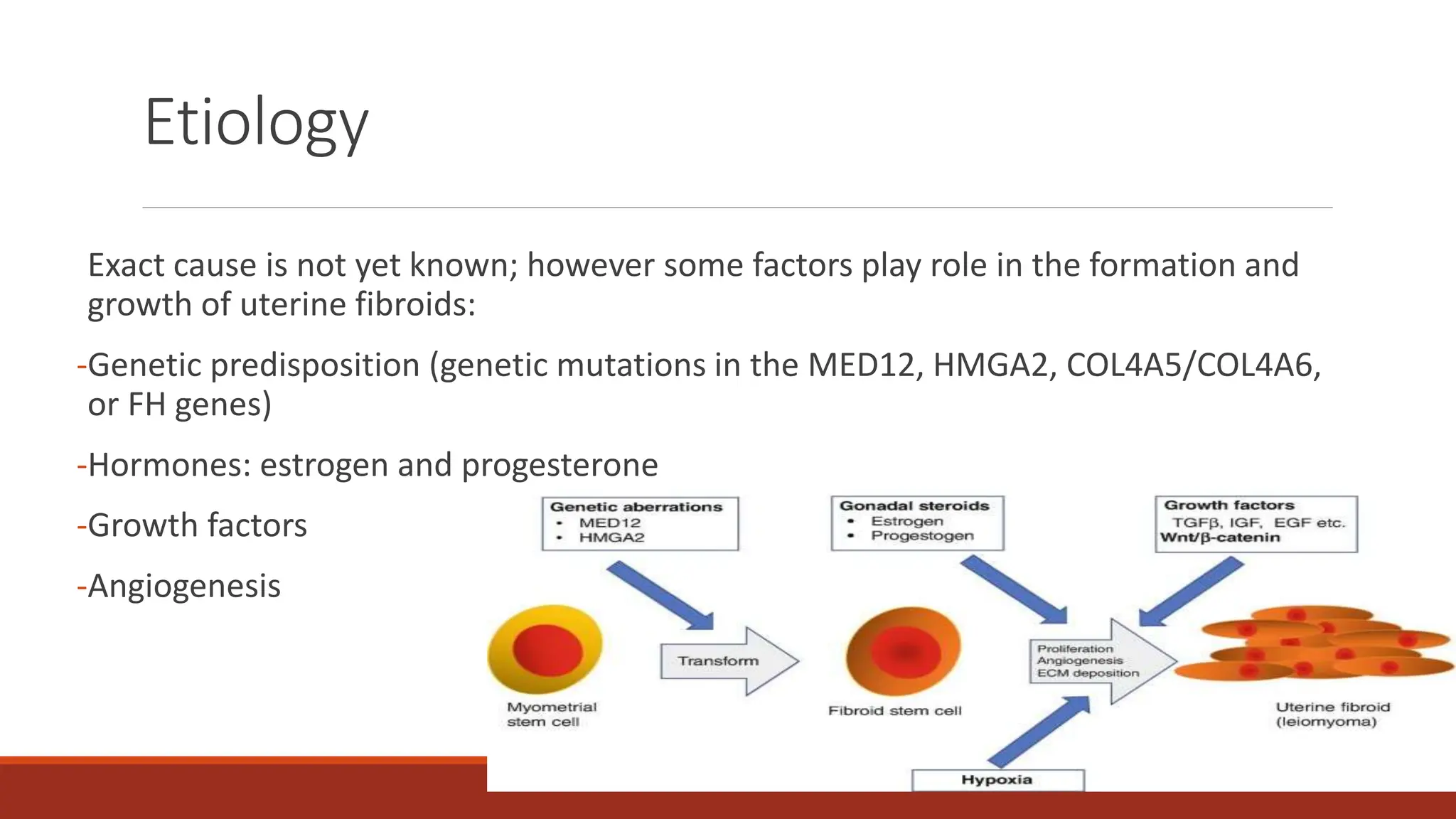
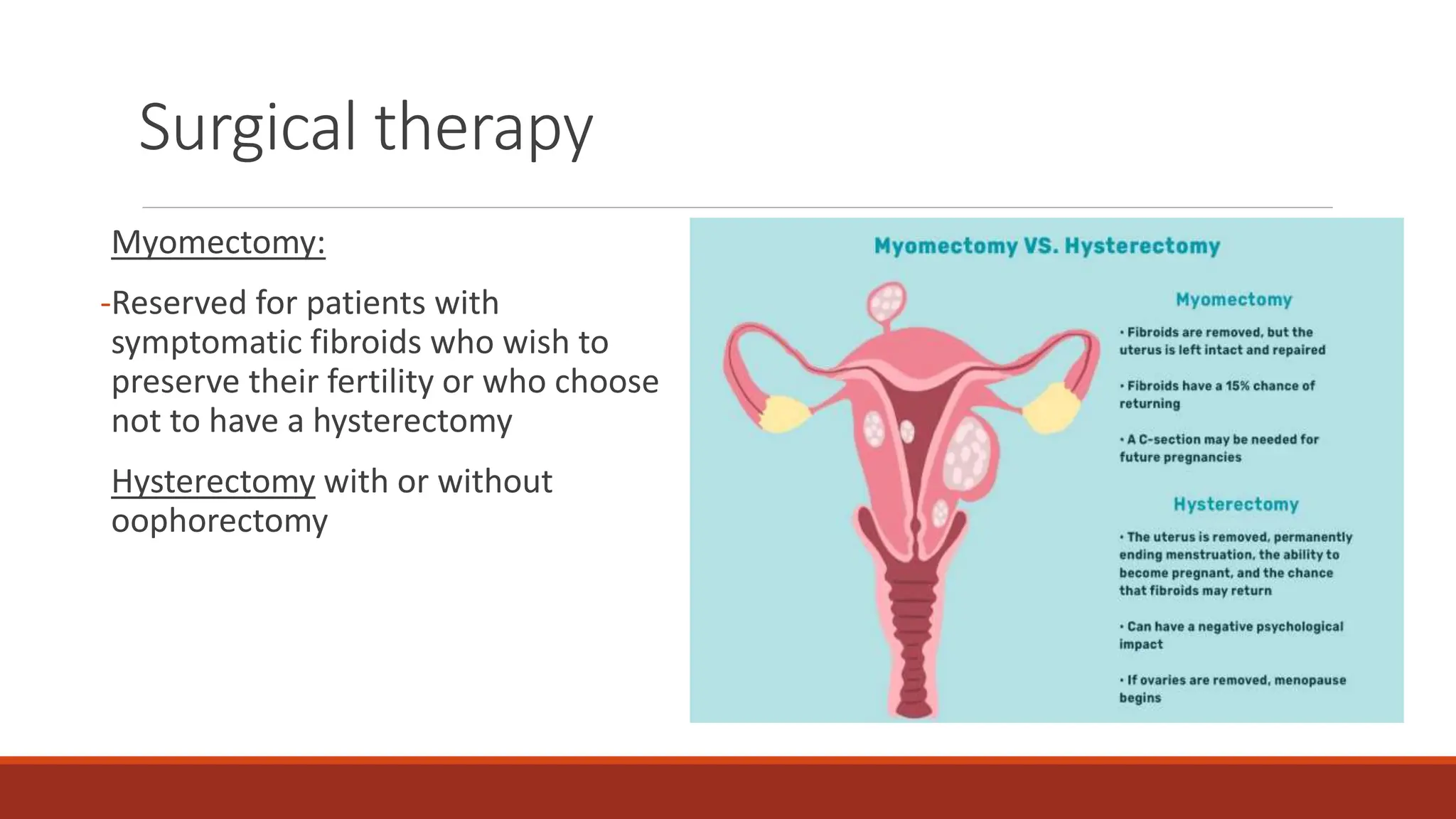
Uterine fibroids are noncancerous tumors that arise from the smooth muscle cells of the uterus. They are the most common benign tumors of the female reproductive system. The exact cause is unknown but factors like genetics, hormones, growth factors, and angiogenesis play a role. Diagnosis involves examinations and imaging tests. Treatment depends on symptoms and may include medical therapy with hormones or procedures like uterine artery embolization or surgery.



































































![menstrual cycle [Autosaved]-2 (5).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/menstrualcycleautosaved-25-230321042311-7c0898c3-thumbnail.jpg?width=640&height=640&fit=bounds)






















