This document provides information on obstetric analgesia techniques for labor pain. It discusses:
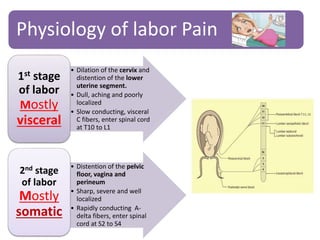
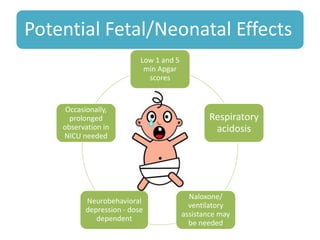
- The physiology of labor pain and its effects on the mother and fetus. Labor pain stimulates the release of hormones that can affect uterine contraction and fetal oxygen levels.
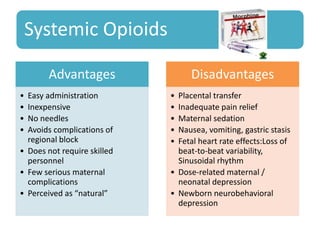
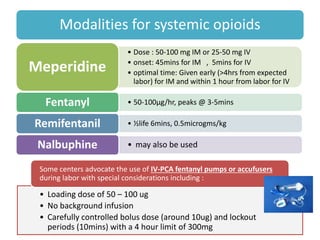
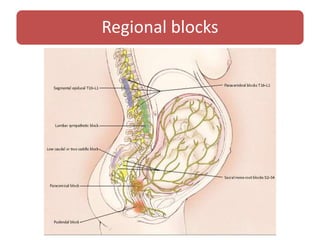
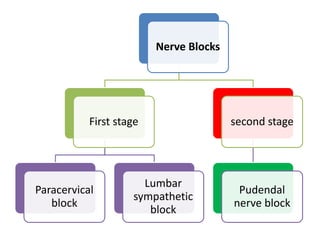
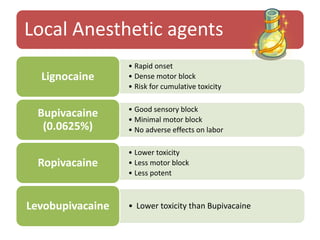
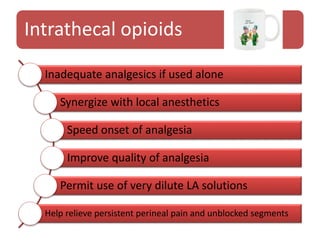
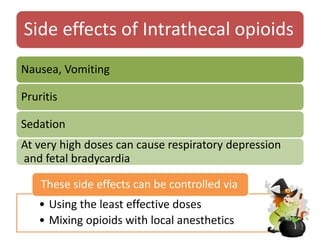
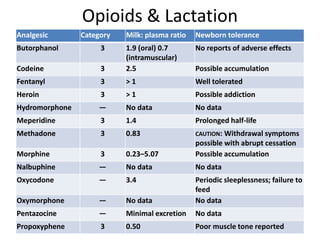
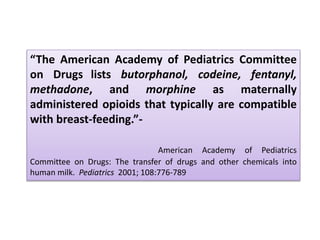
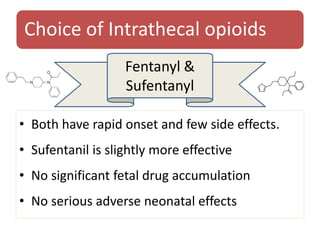
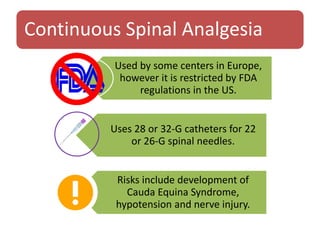
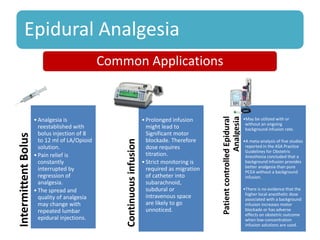
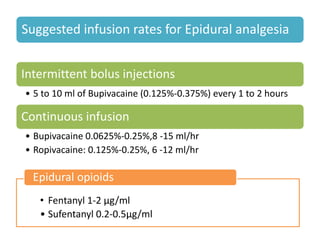
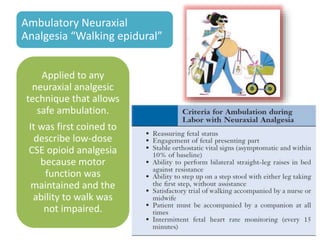
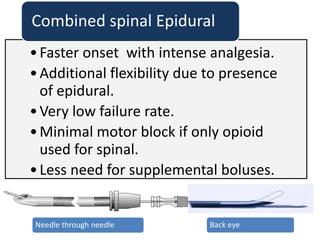
- Various pharmacological and non-pharmacological techniques for pain management, including systemic opioids, inhalational gases, regional nerve blocks, and spinal analgesia using local anesthetics and opioids.
- The advantages and disadvantages of different techniques. Neuraxial blocks like epidurals provide the most effective pain relief with few side effects on the mother or fetus, while minimizing depressant effects seen with systemic opioids.






















![PHYSIOLOGY OF LABOUR PAIN AND LABOUR ANALGESIA [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/physiologyoflabourpainandlabouranalgesiaautosavedautosaved-230406110245-4cf32dcd-thumbnail.jpg?width=640&height=640&fit=bounds)















































