

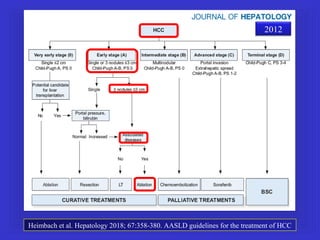
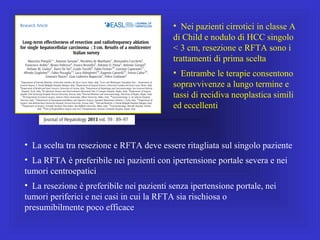
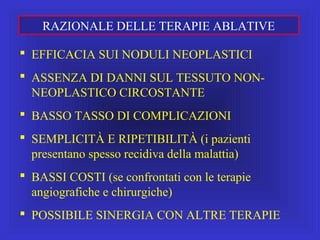


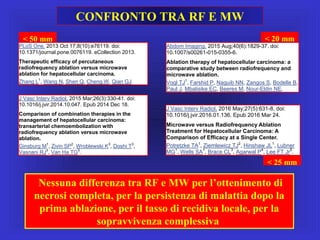


















Il documento descrive le procedure di ecografia operativa in gastroenterologia, evidenziando l'importanza della biopsia ecoguidata per la diagnosi e il trattamento di neoplasie addominali. Le terapie ablative, come la radiofrequenza e l'ablazione a microonde, sono discusse in relazione all'epatocarcinoma, sottolineando la loro efficacia e la necessità di un approccio personalizzato. Inoltre, viene trattato il drenaggio ecoguidato degli ascessi epatici e le tecniche di trattamento per le cisti idatidee.














































