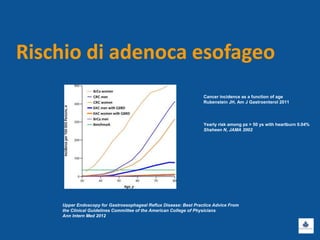
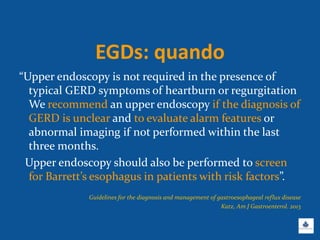

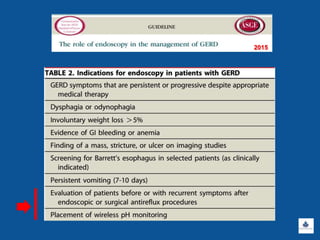
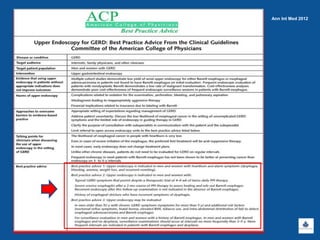




Il documento discute le linee guida e la gestione clinica della malattia da reflusso gastroesofageo (MRGE) e dell'esofago di Barrett, basandosi su raccomandazioni internazionali e dati epidemiologici. Viene evidenziata l'importanza dell'endoscopia per la diagnosi, la sorveglianza e il trattamento, sottolineando l'approccio appropriato per garantire l'uso ottimale delle risorse sanitarie. Infine, si fa riferimento ai rischi e ai costi associati a procedure diagnostiche e terapeutiche non necessarie.



























































