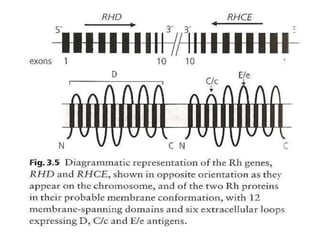
The Rh blood group system is complex, with over 60 antigens identified. The RhD antigen is the most immunogenic after ABO. Individuals are Rh-positive if they possess the D antigen and Rh-negative if they lack it. Weak D variants exist where D antigen expression is reduced, increasing the risk of alloimmunization. The Rh system was initially thought to involve three genes (D, C, E) but genetic studies show it involves two closely linked genes, RHD and RHCE, as well as an associated glycoprotein gene RHAG. Weak D can arise from position effects, quantitative or partial D antigen expression. Ongoing research continues to uncover the genetic complexity of the Rh system.