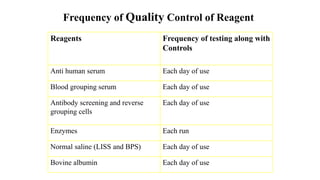
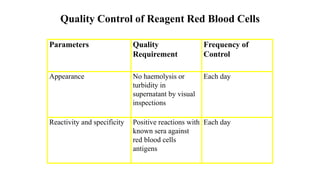
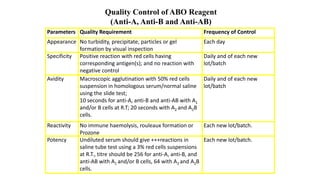
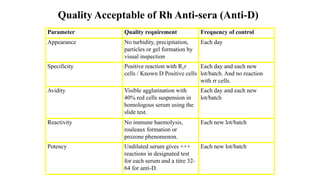
This document discusses quality control in blood banks. It defines quality assurance and quality control, and describes the types of internal and external quality control. It emphasizes the importance of quality control in blood transfusion to ensure safe blood products. It outlines the key steps and parameters involved in quality control for blood collection, testing, component preparation, storage and transportation. These include controls for reagents, equipment, facilities and processes to minimize risks to donors and patients.














































![Introduction to Quality in the Blood Transfusion Service[2].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontoqualityinthebloodtransfusionservice2-241026050402-63b84e56-thumbnail.jpg?width=640&height=640&fit=bounds)

























