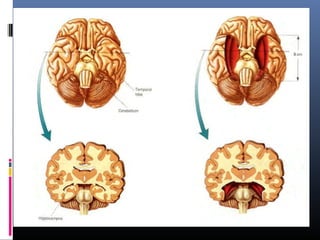
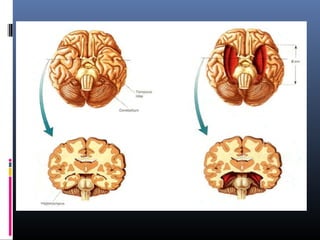
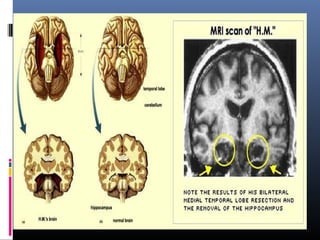
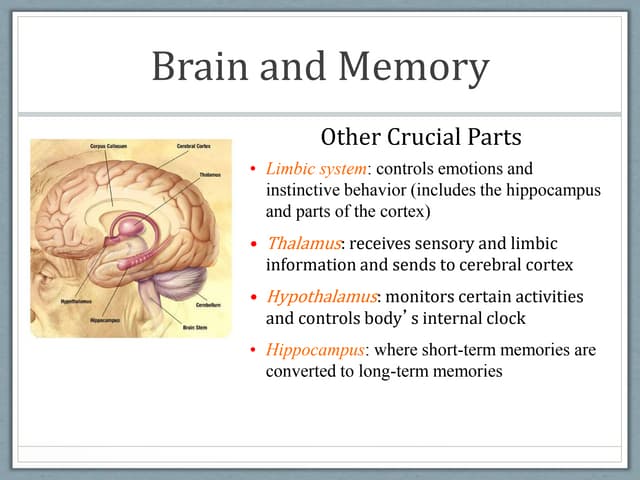
The document discusses learning and memory. It explains that learning involves how experience changes the brain, while memory involves how these changes are stored and retrieved. It describes the different types of memory (sensory, short-term, long-term) and where memories are stored in the brain. The case of patient H.M., who had medial temporal lobe removal, demonstrated the role of these areas in forming new memories and provided evidence for separate short-term and long-term memory systems. Concussions can cause retrograde and anterograde amnesia, providing evidence that memories are consolidated over time.


















































![60)NEUROBIOLOGY_OF_MEMORY[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/60neurobiologyofmemory1-231214020219-bfbe6909-thumbnail.jpg?width=640&height=640&fit=bounds)


























![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)







