The document discusses the neurobiology of memory. It covers:
1. The key stages of memory including encoding, storing, and recall. Immediate, short-term, working, and long-term memory are described.
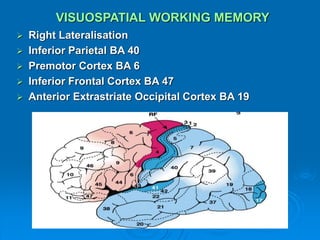
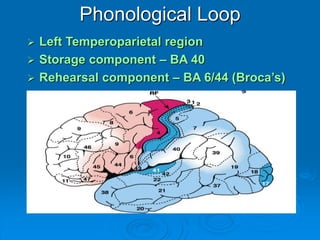
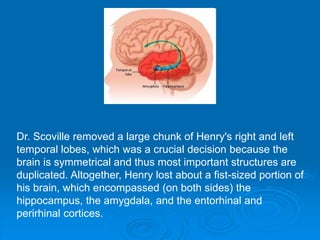
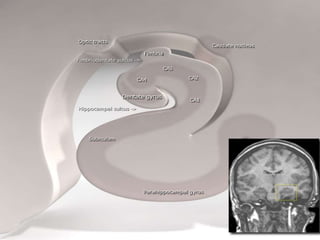
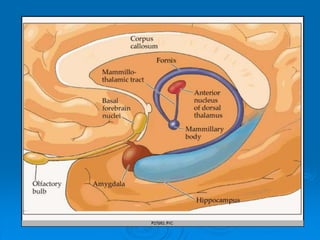
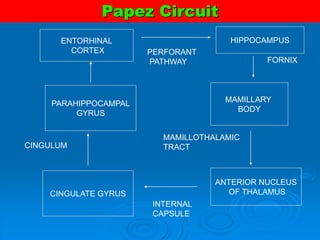
2. The neuroanatomical correlates of memory including the hippocampus, medial diencephalon, basal forebrain, prefrontal cortex, and subcortical nuclei.
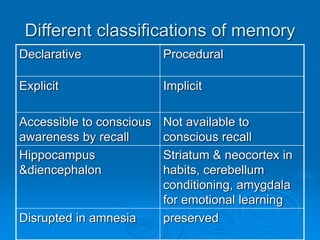
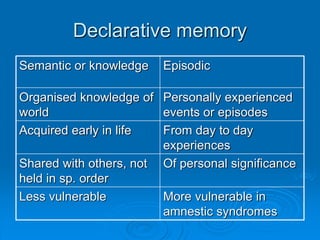
3. Theories of memory such as the consolidation theory and multiple trace theory. Different classifications of memory like declarative vs procedural are also covered.
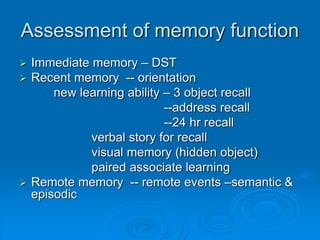
4. Assessment of memory function and various clinical types of memory disorders are discussed like amnesia.