
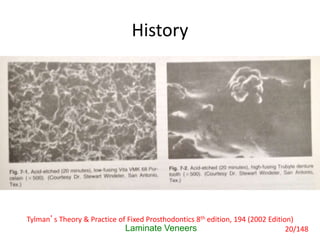
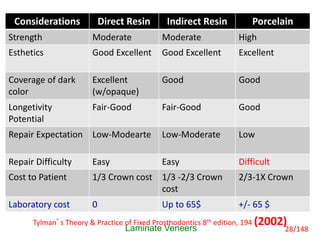
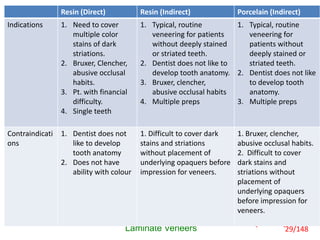
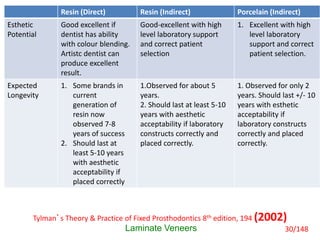
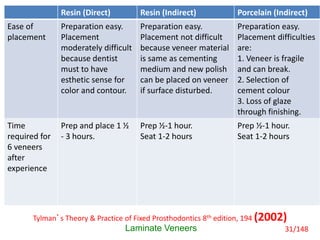
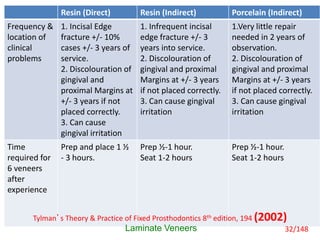
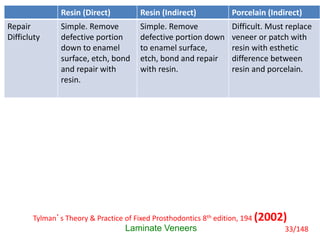




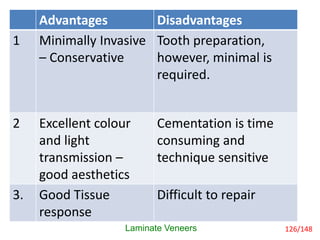
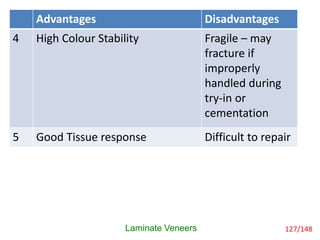
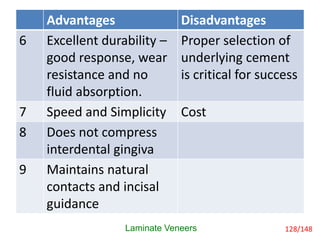







This document discusses laminate veneers, including their history, definitions, indications, contraindications, and comparisons of different types of veneers. Laminate veneers originated in the 1930s when Dr. Charles Pincus used thin resin and porcelain facings to create Hollywood smiles for actors. The document compares direct resin veneers, indirect resin veneers, and porcelain indirect veneers in terms of strength, esthetics, longevity, costs, and other factors. Porcelain indirect veneers generally provide the best esthetics and longevity while direct resin veneers are best for covering dark stains and cost less.

































































































