Downloaded 25 times


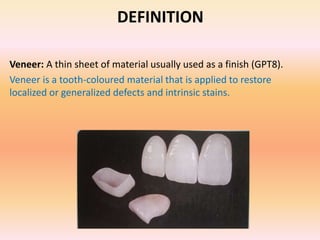











































This document discusses laminate veneers, including: 1. Laminate veneers have evolved over decades to become a popular aesthetic restoration, providing a conservative alternative to full coverage restorations. 2. They involve bonding thin ceramic restorations to etched tooth structure to restore the facial and proximal surfaces. 3. Indications include masking diastemas, discoloration, enamel defects, malpositioned teeth, while contraindications include insufficient tooth structure or parafunctional habits.













































































