Kshivets IASLC 2019
•
276 likes•12,052 views

This study investigated blood cell subpopulations for early detection of lung cancer. It analyzed 115 early stage lung cancer patients and 402 controls, examining various blood factors. Neural network analysis found that lymphocytes, segmented neutrophils, monocytes, eosinophils, and leukocytes were most important for detection. The neural network correctly classified all cases. Bootstrap simulation also identified segmented neutrophils, total segmented neutrophils, lymphocytes, and total leukocytes as significant factors for early lung cancer detection based on blood tests.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Kshivets IASLC 2019
Similar to Kshivets IASLC 2019 (20)
More from Oleg Kshivets
More from Oleg Kshivets (16)
Recently uploaded
Recently uploaded (20)
Kshivets IASLC 2019
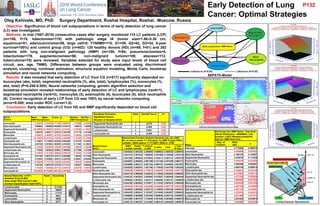
- 1. Early Detection of Lung Cancer: Optimal Strategies Oleg Kshivets, MD, PhD Surgery Department, Roshal Hospital, Roshal, Moscow, Russia Objective: Significance of blood cell subpopulations in terms of early detection of lung cancer (LC) was investigated. Methods: In trial (1987-2019) consecutive cases after surgery, monitored 115 LC patients (LCP) (m=100, f=15; lobectomies=115) with pathologic stage IA (tumor size=1.86±0.30 cm; squamous=51, adenocarcinoma=59, large cell=5; T1N0M0=115; G1=39, G2=42, G3=34, 5-year survival=100%) and control group (CG) (n=402): 120 healthy donors (HD) (m=69, f=51) and 282 patients with lung non-malignant pathology (NMP) (m=188, f=94; pneumonectomies=5, lobectomies=179, segmentectomies=98; non-malignant tumors=100; abscess=112; tuberculoma=70) were reviewed. Variables selected for study were input levels of blood cell circuit, sex, age, TNMG. Differences between groups were evaluated using discriminant analysis, clustering, nonlinear estimation, structural equation modeling, Monte Carlo, bootstrap simulation and neural networks computing. Results: It was revealed that early detection of LC from CG (n=517) significantly depended on: leucocytes (abs, total), segmented neutrophils (%, abs, total), lymphocytes (%), monocytes (%, abs, total) (P=0.048-0.000). Neural networks computing, genetic algorithm selection and bootstrap simulation revealed relationships of early detection of LC and lymphocytes (rank=1), segmented neutrophils (rank=2), monocytes (3), eosinophils (4), leucocytes (5), stick neutrophils (6). Correct recognition of early LCP from CG was 100% by neural networks computing (error=0.000; area under ROC curve=1.0). Conclusion: Early detection of LC from HD and NMP significantly depended on blood cell subpopulations. Blood Factors Mean NMP+Norm Mean Cancer t-value p Std.Dev. NMP+Norm Std.Dev. Cancer Leucocytes 5.32015 5.87043 -2.71185 0.006915 1.78399 2.33204 Stick Neutrophils 0.99502 1.09565 -0.64469 0.519414 1.50973 1.35059 Segmented Neutrophils 58.39055 61.46087 -2.53241 0.011624 11.55100 11.15622 Eosinophils 3.56219 3.05617 1.37675 0.169188 3.71119 2.47445 Monocytes 2.94527 3.46087 -1.97725 0.048546 2.32024 2.92085 Lymphocytes 34.19403 30.94783 2.75936 0.005998 11.23262 10.73594 Eosinophils abs 0.18837 0.17902 0.43436 0.664208 0.21370 0.16201 Stick Neutrophils abs 0.05749 0.07092 -1.09385 0.274532 0.11302 0.12631 Segmented Neutrophils abs 3.14426 3.60482 -3.10649 0.001998 1.36638 1.52038 Lymphocytes abs 1.77649 1.80523 -0.30561 0.760026 0.77289 1.21320 Monocytes abs 0.15535 0.21188 -3.36648 0.000818 0.13944 0.21328 Eosinophils tot 0.91769 0.86378 0.51673 0.605569 1.03943 0.77206 Stick Neutrophils tot 0.27943 0.35086 -1.22613 0.220709 0.52941 0.62059 Segmented Neutrophils tot 15.30056 17.73777 -3.16338 0.001652 7.03675 8.09992 Lymphocytes tot 8.62168 8.80075 -0.37016 0.711413 4.09357 5.96624 Monocytes tot 0.75284 1.04564 -3.55172 0.000418 0.68479 1.04679 Leucocytes tot 25.85628 28.79386 -2.68146 0.007565 9.74573 12.27662 Blood Factors N=517 Discriminant Function Analysis Summary (elc_dp_n002) No. of vars in model: 17; Grouping: Ca_NMP (2 grps) Wilks' Lambda: .93942 approx. F (17,499)=1.8928 p< .0166 Wilks' Lambda Partial Lambda F-remove (1,499) p-value Toler. 1-Toler. (R-Sqr.) Leucocytes 0.945636 0.993430 3.299895 0.069884 0.000030 0.999970 Stick Neutrophils 0.941472 0.997824 1.088048 0.297409 0.108486 0.891514 Segmented Neutrophils 0.941266 0.998043 0.978654 0.323011 0.004721 0.995279 Eosinophils 0.944501 0.994624 2.697189 0.101155 0.031829 0.968171 Monocytes 0.944698 0.994417 2.801764 0.094787 0.048493 0.951507 Lymphocytes 0.942826 0.996391 1.807346 0.179438 0.004708 0.995292 Eosinophils abs 0.948309 0.990630 4.719812 0.030287 0.002269 0.997731 Stick Neutrophils abs 0.944118 0.995028 2.493570 0.114946 0.004633 0.995367 Segmented Neutrophils abs 0.945233 0.993854 3.085688 0.079597 0.000056 0.999944 Lymphocytes abs 0.946093 0.992951 3.542417 0.060400 0.000137 0.999864 Monocytes abs 0.944160 0.994983 2.515877 0.113338 0.003474 0.996526 Eosinophils tot 0.947924 0.991032 4.515480 0.034080 0.002778 0.997222 Stick Neutrophils tot 0.943604 0.995569 2.220710 0.136802 0.005169 0.994831 Segmented Neutrophils tot 0.945435 0.993641 3.193357 0.074545 0.000057 0.999943 Lymphocytes tot 0.946065 0.992980 3.527546 0.060940 0.000143 0.999857 Monocytes tot 0.941900 0.997370 1.315639 0.251926 0.003925 0.996075 Leucocytes tot 0.945715 0.993347 3.341892 0.068134 0.000028 0.999972 Effect All Groups Ca—NMP+Norm - Test of all effects Distribution : BINOMIAL, Link function: LOGIT Modeled probability that Ca—NMP+Norm=Ca Degr. of Freedom Wald Stat. p Intercept 1 2.770466 0.096018 Leucocytes 1 4.424666 0.035423 Stick Neutrophils 1 2.169120 0.140807 Segmented Neutrophils 1 2.539519 0.111029 Eosinophils 1 5.206370 0.022504 Monocytes 1 3.465356 0.062667 Lymphocytes 1 3.564749 0.059019 Eosinophils abs 1 5.786612 0.016149 Stick Neutrophils abs 1 4.212904 0.040118 Segmented Neutrophils abs 1 4.277158 0.038628 Lymphocytes abs 1 4.608960 0.031805 Monocytes abs 1 3.934539 0.047304 Eosinophils tot 1 5.587765 0.018086 Stik Neutrophils tot 1 4.061129 0.043881 Segmented Neutrophils tot 1 4.379579 0.036372 Lymphocytes tot 1 4.621466 0.031574 Monocytes tot 1 3.281245 0.070076 Leucocytes tot 1 4.482998 0.034234 Neural Networks: n=517; Baseline Error=0.000; Area under ROC Curve=1.000; Correct Classification Rate=100% Rank Sensitivity Lymphocytes 1 211222 Segmented Neutrophils 2 16605 Monocytes 3 11174 Eosinophils 4 9421 Leucocytes 5 9065 Stick Neutrophils 6 8777 Bootstrap Simulation Significant Factors (Number of Samples=3333) Rank Kendall’Tau-A P< Segmented Neutrophils abs 1 -0.075 0.05 Segmented Neutrophils tot 2 -0.069 0.05 Lymphocytes 3 0.063 0.05 Leucocytes tot 4 -0.059 0.05 P132