Kshivets iaslc toronto2018
•
280 likes•10,787 views

1) The study investigated the significance of blood cell levels in early detection of lung cancer by analyzing data from 115 lung cancer patients and 120 healthy individuals. 2) Neural network analysis revealed that early lung cancer detection depended most on lymphocyte levels, followed by neutrophil levels, monocytes, and other blood cells. 3) The neural networks achieved 100% accurate detection of early lung cancer based on blood cell levels, demonstrating their potential for precise early detection.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Kshivets iaslc toronto2018
Similar to Kshivets iaslc toronto2018 (20)
More from Oleg Kshivets
More from Oleg Kshivets (15)
Recently uploaded
Recently uploaded (20)
Kshivets iaslc toronto2018
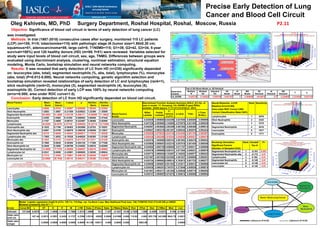
- 1. Precise Early Detection of Lung Cancer and Blood Cell Circuit Oleg Kshivets, MD, PhD Surgery Department, Roshal Hospital, Roshal, Moscow, Russia P2.11 Objective: Significance of blood cell circuit in terms of early detection of lung cancer (LC) was investigated. Methods: In trial (1987-2018) consecutive cases after surgery, monitored 115 LC patients (LCP) (m=100, f=15; lobectomies=115) with pathologic stage IA (tumor size=1.86±0.30 cm; squamous=51, adenocarcinoma=59, large cell=5; T1N0M0=115; G1=39, G2=42, G3=34, 5-year survival=100%) and 120 healthy donors (HD) (m=69, f=51) were reviewed. Variables selected for study were input levels of blood cell circuit, sex, age, TNMG. Differences between groups were evaluated using discriminant analysis, clustering, nonlinear estimation, structural equation modeling, Monte Carlo, bootstrap simulation and neural networks computing. Results: It was revealed that early detection of LC from HD (n=235) significantly depended on: leucocytes (abs, total), segmented neutrophils (%, abs, total), lymphocytes (%), monocytes (abs, total) (P=0.012-0.000). Neural networks computing, genetic algorithm selection and bootstrap simulation revealed relationships of early detection of LC and lymphocytes (rank=1), stick neutrophils (rank=2), monocytes (3), segmented neutrophils (4), leucocytes (5), eosinophils (6). Correct detection of early LCP was 100% by neural networks computing (error=0.000; area under ROC curve=1.0). Conclusion: Early detection of LC from HD significantly depended on blood cell circuit. Blood Factors Mean - Norm Mean - Cancer t-value p Std.Dev. - Norm Std.Dev. - Cancer Leucocytes 4.9650 5.8704 -3.49567 0.000566 1.58240 2.33204 Stick Neutrophils 1.0583 1.0957 -0.21389 0.830823 1.32396 1.35059 Segmented Neutrophils 55.8583 61.4609 -3.93139 0.000111 10.68990 11.15622 Eosinophils 3.2250 3.0562 0.41205 0.680682 3.66556 2.47445 Monocytes 3.1167 3.4609 -0.99151 0.322467 2.38406 2.92085 Lymphocytes 36.8250 30.9478 4.27742 0.000028 10.32714 10.73594 Eosinophils abs 0.1632 0.1790 -0.59403 0.553066 0.23783 0.16201 Stick Neutrophils abs 0.0591 0.0709 -0.86079 0.390238 0.08058 0.12631 Segmented Neutrophils abs 2.8110 3.6048 -4.48441 0.000011 1.17819 1.52038 Lymphocytes abs 1.7805 1.8052 -0.19326 0.846926 0.68395 1.21320 Monocytes abs 0.1532 0.2119 -2.54010 0.011733 0.13311 0.21328 Eosinophils tot 0.7865 0.8638 -0.59394 0.553125 1.17369 0.77206 Stick Neutrophils tot 0.2848 0.3509 -0.96799 0.334052 0.40818 0.62059 Segmented Neutrophils tot 13.4859 17.7378 -4.58500 0.000007 6.00216 8.09992 Lymphocytes tot 8.5241 8.8008 -0.43961 0.660628 3.38285 5.96624 Monocytes tot 0.7315 1.0456 -2.76601 0.006130 0.65846 1.04679 Leucocytes tot 23.8069 28.7939 -3.66118 0.000311 8.30366 12.27662 Blood Factors N=235 Discriminant Function Analysis Summary (EDLC_N1) No. of vars in model: 17; Grouping: CA--NORM (2 grps) Wilks' Lambda: .83538 approx. F (17,217)=2.5155 p< .0012 Wilks' Lambda Partial Lambda F- remove (1,217) p-value Toler. 1-Toler. (R-Sqr.) Leucocytes 0.835539 0.999805 0.042398 0.837055 0.000005 0.999995 Stick Neutrophils 0.847328 0.985894 3.104805 0.079470 0.031455 0.968545 Segmented Neutrophils 0.848397 0.984652 3.382399 0.067262 0.000486 0.999514 Eosinophils 0.849547 0.983319 3.681257 0.056340 0.005576 0.994424 Monocytes 0.852830 0.979533 4.534138 0.034352 0.007193 0.992807 Lymphocytes 0.850429 0.982299 3.910244 0.049258 0.000521 0.999479 Eosinophils abs 0.835376 1.000000 0.000103 0.991893 0.000478 0.999522 Stick Neutrophils abs 0.835500 0.999851 0.032310 0.857518 0.001454 0.998546 Segmented Neutrophils abs 0.835594 0.999738 0.056859 0.811757 0.000011 0.999989 Lymphocytes abs 0.835476 0.999880 0.026101 0.871804 0.000021 0.999979 Monocytes abs 0.835773 0.999524 0.103267 0.748253 0.000577 0.999423 Eosinophils tot 0.837467 0.997502 0.543392 0.461827 0.000609 0.999391 Stick Neutrophils tot 0.835724 0.999583 0.090514 0.763813 0.001723 0.998277 Segmented Neutrophils tot 0.839000 0.995681 0.941352 0.333011 0.000012 0.999988 Lymphocytes tot 0.838435 0.996351 0.794781 0.373646 0.000026 0.999974 Monocytes tot 0.841001 0.993311 1.461255 0.228046 0.000718 0.999282 Leucocytes tot 0.838741 0.995987 0.874275 0.350814 0.000006 0.999994 N=235 Model: Logistic regression (logit) N of 0's: 120 1's: 115 Dep. var: Ca-Norm Loss: Max likelihood Final loss: 140.17256193 Chi2 (17)=45.328 p=.00022 Modeled probability that ST = 1. Const.B0 L ST S E M LYM Eabs STabs Sabs LYMabs Mabs Etot STtot Stot LYMtot Mtot Ltot Estimate 137.845 6.0578 -1.27 -1.3505 -1.4148 -1.7565 -1.4314 1.3690 10.7 -7.347 -4.1421 -12.05 4.7529 1.586 6.4389 5.8372 9.194 -6.1893 Odds ratio (unit ch) 427.44 0.2813 0.2591 0.2430 0.1727 0.2390 3.9315 42852 0.0006 0.01589 0.000 115.92 4.882 625.739 342.809 9842.75 0.0021 Odds ratio (range) 0.0005 0.0000 0.0000 0.0000 0.0000 19.136 138511 0.000 0.0000 0.000 5563.08 0.0000 Dependent Variable Test of SS Whole Model vs. SS Residual Multiple R Multiple R2 Adjusted R2 SS Model df Model MS Model SS Residual df Residual MS Residual F p CA_NORM 0.405739 0.164624 0.099180 9.667307 17 0.568665 49.05610 217 0.226065 2.515494 0.001154 Neural Networks: n=235 Baseline Error=0.000; Area under ROC Curve=1.000; Correct Classification Rate=100% Rank Sensitivity Lymphocytes 1 3076 Stick Neutrophils 2 2323 Monocytes 3 2216 Segmented Neutrophils 4 2018 Leucocytes 5 1917 Eosinophils 6 1771 Bootstrap Simulation Significant Factors (Number of Samples=3333) Rank Kendall’ Tau-A P< Segmented Neutrophils tot 1 -0.191 0.001 Segmented Neutrophils abs 2 -0.172 0.01 Lymphocytes 3 0.162 0.01 Segmented Neutrophils 4 -0.149 0.01 Leucocytes tot 5 -0.140 0.01 Leucocytes 6 -0.125 0.01