Kshivets aats new_york2018
•
281 likes•12,077 views

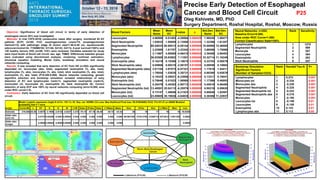
Precise Early Detection of Esophageal Cancer and Blood Cell Circuit
Report
Share
Report
Share
Download to read offline
Recommended
Kshivets O. Lung Cancer: Early Detection and Diagnosis 
Lung Cancer: Early Detection and Diagnosis and Immune System
Kshivets IASLC_Vienna2016
5-Year Survival of Lung Cancer Patients after Radical Surgery was Significantly Depended on Tumor Characteristics, Blood Cell Circuit, Cell Ratio Factors, Hemostasis System, Biochemic Homeostasis, Surgery Type, Adjuvant Treatment and Anthropometric Data
Kshivets iaslc denver2015
PRECISE PREDICTION OF 5-YEAR SURVIVAL OF LUNG CANCER PATIENTS AFTER RADICAL SURGERY
Kshivets barcelona2016
5-Year Survival of Gastric Cancer Patients after Radical Surgery was Significantly Depended on Tumor Characteristics, Blood Cell Circuit, Cell Ratio Factors, Hemostasis System and Adjuvant Treatment
Kshivets O. Lung Cancer Surgery: Prognosis
HOMEOSTASIS NETWORKS IN PROGNOSIS OF LUNG CANCER PATIENTS SURVIVAL
Recommended
Kshivets O. Lung Cancer: Early Detection and Diagnosis
Lung Cancer: Early Detection and Diagnosis and Immune System
Kshivets IASLC_Vienna2016
5-Year Survival of Lung Cancer Patients after Radical Surgery was Significantly Depended on Tumor Characteristics, Blood Cell Circuit, Cell Ratio Factors, Hemostasis System, Biochemic Homeostasis, Surgery Type, Adjuvant Treatment and Anthropometric Data
Kshivets iaslc denver2015
PRECISE PREDICTION OF 5-YEAR SURVIVAL OF LUNG CANCER PATIENTS AFTER RADICAL SURGERY
Kshivets barcelona2016
5-Year Survival of Gastric Cancer Patients after Radical Surgery was Significantly Depended on Tumor Characteristics, Blood Cell Circuit, Cell Ratio Factors, Hemostasis System and Adjuvant Treatment
Kshivets O. Lung Cancer Surgery: Prognosis
HOMEOSTASIS NETWORKS IN PROGNOSIS OF LUNG CANCER PATIENTS SURVIVAL
Kshivets O. Lung Cancer Surgery
Immunologic Predictors of the Risc of Generalization in Non-Small Cell Lung Cancer Patients after Comlete Resections
Kshivets milan2014
5-YEAR SURVIVAL OF UPPER THIRD ESOPHAGEAL CANCER PATIENTS WAS SIGNIFICANTLY SUPERIOR IN COMPARISON WITH MIDDLE AND LOWER THIRD ESOPHAGEAL CANCER PATIENTS AFTER RADICAL SURGERY AND STRONGLY DEPENDED ON PHASE TRANSITION EARLY-INVASIVE CANCER, LYMPH NODE METASTASES, CELL RATIO FACTORS AND ADJUVANT CHEMOIMMUNORADIOTHERAPY
Kshivets O. Lung Cancer Surgery
NEURAL NETWORKS AND BOOTSTRAP SIMULATION IN PREDICTION OF OUTCOME OF NON-SMALL CELL LUNG CANCER PATIENTS AFTER COMPLETE LOBECTOMIES AND PNEUMONECTOMIES
Kshivets iaslc denver2021
Lung Cancer Prognosis and Cell Ratio Factors
OBJECTIVE: We examined cell ratio factors (CRF) significantly affecting non-small cell lung cancer (LC) patients (LCP) survival. CRF - ratio between cancer cells (CC) and blood cells subpopulations.
Cox modeling displayed that LCP survival significantly depended on CRF: leucocytes/CC, segmented neutrophils/CC, lymphocytes/CC, healthy cells/CC (P=0.000-0.016). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and healthy cells/CC (rank=1), segmented neutrophils/CC (rank=2), erythrocytes/CC (rank=3), thrombocytes/CC (4), leucocytes/CC (5), lymphocytes/CC (6), eosinophils/CC (7), monocytes/CC (8), stick neutrophils/CC (9). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: LCP survival after radical procedures significantly depended on CRF.
Kshivets iaslc singapore2020
Lymph Node Metastases of Lung Cancer and Blood Cell Circuit
Kshivets Oleg Surgery Department, Roshal Hospital, Moscow, Russia
OBJECTIVE: Significance of blood cell circuit in terms of detection of non-small cell lung cancer (LC) patients (LCP) with lymph node metastases was investigated.
METHODS: We analyzed data of 757 consecutive LCP (age=57.6±8.2 years; tumor size=4.1±2.4 cm) radically operated (R0) and monitored in 1985-2020 (m=654, f=103; upper lobectomies=272, lower lobectomies=176, middle lobectomies=18, bilobectomies=42, pneumonectomies=249, mediastinal lymph node dissection=757; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=192; T1=317, T2=251, T3=132, T4=57; N0=509, N1=130, N2=118, M0=757; G1=194, G2=238, G3=325; squamous=415, adenocarcinoma=292, large cell=50. Variables selected for study were input levels of blood cell circuit, sex, age, TNMG. Differences between groups were evaluated using discriminant analysis, clustering, nonlinear estimation, structural equation modeling, Monte Carlo, bootstrap simulation and neural networks computing.
RESULTS: It was revealed that separation of LCP with lymph node metastases (n=248) from LCP without metastases (n=509) significantly depended on: leucocytes (abs, total), segmented neutrophils (%, abs, total), lymphocytes (%), ESS, Rh, coagulation time, prothrombin index, fibrinogen, heparin tolerance, cell ratio factors (CRF) (ratio between cancer cells- CC and blood cells subpopulations), T, G, tumor size (P=0.047-0.000). Neural networks computing, genetic algorithm selection and bootstrap simulation revealed relationships of lymph node metastases and CRF: healthy cells/CC (rank=1), segmented neutrophils/CC (2), leucocytes/CC (3), erythrocytes/CC (4), lymphocytes/CC (5), thrombocytes/CC (6), eosinophils/CC (7), monocytes/CC (8), stick neutrophils/CC (9). Correct classification N0—N12 was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSION: Lymph node metastases significantly depended on blood cell circuit.
PRECISE EARLY DETECTION OF LUNG CANCER AND IMMUNE CIRCUIT
PRECISE EARLY DETECTION OF LUNG CANCER AND IMMUNE CIRCUIT
Kshivets wscts2015
Artificial Intelligence, System Analysis and Simulation Modeling in Precise Prediction of 5-Year Survival of Esophageal Cancer Patients after Complete Esophagogastrectomies
Kshivets aats new_york2019
Survival of Esophageal Cancer Patients was Significantly Superior in Comparison with Cardioesophageal Cancer Patients after Surgery
Kshivets Oleg Surgery Department, Roshal Hospital, Moscow, Russia
OBJECTIVE: This study aimed to determine localization influence of tumor for 5-year survival (5YS) of esophageal (EC) or cardioesophageal (CC) cancer patients (ECP, CEP) after complete en block (R0) esophagogastrectomies (EG) through left/right thoracoabdominal incision.
METHODS: We analyzed data of 543 consecutive patients (age=56.4±8.8 years; tumor size=6±3.5 cm) radically operated (R0) and monitored in 1975-2019 (m=405, f=138; ECP=259, CEP=284; esophagogastrectomies (EG) Garlock=280, EG Lewis=263, combined EG with resection of pancreas, liver, diaphragm, aorta, VCS, colon transversum, lung, trachea, pericardium, splenectomy=151; adenocarcinoma=308, squamous=225, mix=10; T1=126, T2=114, T3=178, T4=125; N0=275, N1=69, N2=199; G1=157, G2=139, G3=247; early EC=107, invasive=436; only surgery=420, adjuvant chemoimmunoradiotherapy-AT=123: 5-FU+thymalin/taktivin+radiotherapy 45-50Gy). Multivariate Cox modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 1892.4±2241 days and cumulative 5-year survival (5YS) reached 51.9%, 10 years – 45.7%, 20 years – 33.5%. 183 ECP lived more than 5 years (LS=4311±2419.7 days), 98 ECP – more than 10 years (LS=5903.4±2299.4 days). 224 died because of EC/CC (LS=629.2±320.1 days). 5YS of ECP (67.3%, LS=2605±2628.9 days) was significantly superior in comparison with CEP (36.4%, LS=1242.6±1558.5 days) (P=0.00000 by log-rank test). AT significantly improved 5YS (68.2% vs. 48.5%) (P=0.00033 by log-rank test). Cox modeling displayed that 5YS of ECP/CEP significantly depended on: phase transition (PT) N0—N12 in terms of synergetics, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), T, G, histology, age, AT, localization, blood cells, prothrombin index, coagulation time, residual nitrogen, blood group, Rh, glucose, protein (P=0.000-0.008). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and healthy cells/CC (rank=1), PT early-invasive EC (rank=2), PT N0—N12 (rank=3), erythrocytes/CC (4), thrombocytes/CC (5), stick neutrophils/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), eosinophils/CC (9), leucocytes/CC (10), monocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
Kshivets Hong Kong Sydney2020
Combined Lobectomies and Pneumonectomies: Survival Outcomes in Patients with Local Advanced Lung Cancer
Kshivets O. Esophageal & Cardioesophageal Cancer Surgery
ADJUVANT CHEMOIMMUNORADIO/CHEMOIMMUNOTHERAPY SIGNIFICANTLY IMPROVED 5-YEAR SURVIVAL OF ESOPHAGEAL/CARDIOESOPHAGEAL CANCER PATIENTS AFTER RADICAL SURGERY
Kshivets eacts milan2018
Survival Outcomes in Patients with Esophageal Cancer after Complete Esophagogastrectomies
Kshivets O. Lung Cancer Surgery
5-Year Survival of Non-Small Cell Lung Cancer Patients after Radical Surgery Significantly Depended on Phase Transition “Early-Invasive Cancer”, Lymph Node Metastases and Cell Ratio Factors
Kshivets O. Lung Cancer Stage III Surgery
PREDICTION OF 5-YEAR SURVIVAL OF NON-SMALL CELL LUNG CANCER PATIENTS WITH STAGE III AFTER COMPLETE RESECTIONS
Combined Esophagogastrectomies: Survival Outcomes in Patients with Local Adva...
CONCLUSIONS: 5YS of local advanced ECP after combined radical procedures significantly depended on: tumor characteristics, blood cell circuit, cell ratio factors, biochemical factors, hemostasis system, anthropometric data and adjuvant treatment. Optimal strategies for local advanced ECP are: 1) availability of very experienced thoracoabdominal surgeons because of complexity radical procedures; 2) aggressive en block surgery and adequate lymph node dissection for completeness; 3) precise prediction; 4) AT for ECP with unfavorable prognos
Kshivets O. Esophagogastric Cancer Surgery
ARTIFICIAL INTELLIGENCE, SYSTEM ANALYSIS AND SIMULATION MODELING IN OPTIMIZATION OF TREATMENT FOR ESOPHAGOGASTRIC CANCER PATIENTS
Lung Cancer: 10-Year Survival
CONCLUSIONS: 10-Year survival of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) anthropometric data; 10) surgery type; 11) tumor localization. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Esophageal Cancer: Artificial Intelligence, Synergetics, Complex System Analy...
5-year survival of ECP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC cell dynamics; 9) EC characteristics; 10) tumor localization; 11) anthropometric data; 12) surgery type. Optimal diagnosis and treatment strategies for EC are: 1) screening and early detection of EC; 2) availability of experienced thoracoabdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for ECP with unfavorable prognosis.
Kshivets Oleg Optimization of Management for Esophageal Cancer Patients (T1-...
Optimization of Management for Esophageal Cancer Patients (T1-4N0-2M0).
Kshivets Oleg Surgery Department, Bagrationovsk Hospital, Bagrationovsk, Kaliningrad, Russia
ABSTRACT
OBJECTIVE: 5-survival (5YS) and life span after radical surgery for esophageal cancer (EC) pa¬tients (ECP)(T1-4N0-2M0) - alive supersysems was analyzed. The importance must be stressed of using complex system analysis, artificial intelligence (neural networks computing), simulation modeling and statistical methods in combination, because the different approaches yield complementary pieces of prognostic information.
METHODS: We analyzed data of 563 consecutive ECP (age=56.6±8.9 years; tumor size=6±3.5 cm) radically operated (R0) and monitored in 1975-2024 (m=419, f=144; esophagogastrectomies (EG) Garlock=289, EG Lewis=274, combined EG with resection of pancreas, liver, diaphragm, aorta, VCS, colon transversum, lung, trachea, pericardium, splenectomy=170; adenocarcinoma=323, squamous=230, mix=10; T1=131, T2=119, T3=185, T4=128; N0=285, N1=71, N2=207; G1=161, G2=143, G3=259; early EC=112, invasive=451; only surgery=428, adjuvant chemoimmunoradiotherapy-AT=135: 5-FU+thymalin/taktivin+radiotherapy 45-50Gy). Multivariate Cox modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 1915.4±2284.8 days and cumulative 5-year survival (5YS) reached 52.6%, 10 years – 46.3%, 20 years – 33.3%, 30 years – 27.5%. 193 ECP lived more than 5 years (LS=4309.1±2507.4 days), 105 ECP – more than 10 years (LS=5860.8±2469.2 days). 228 ECP died because of EC (LS=629.8±324.1 days). AT significantly improved 5YS (69% vs. 49.1%) (P=0.0007 by log-rank test). 5YS of ECP of upper/3 was significantly better than others (65.3% vs.50.3%) (P=0.003). Cox modeling displayed that 5YS of ECP significantly depended on: phase transition (PT) N0—N12 in terms of synergetics, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), T, G, histology, age, AT, localization, prothrombin index, hemorrhage time, residual nitrogen, protein (P=0.000-0.019). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and healthy cells/CC (rank=1), PT N0—N12 (2), PT early-invasive EC (3), erythrocytes/CC (4), thrombocytes/CC (5); segmented neutrophils/CC (6), stick neutrophils/CC (7), lymphocytes/CC (8), eosinophils/CC (9), monocytes/CC (10), leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5-year survival of ECP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC cell dynamics; 9) EC characteristics; 10) tumor localization; 11) anthropometric data; 12) surgery type. Optimal diagnosis and trea
More Related Content
What's hot
Kshivets O. Lung Cancer Surgery
Immunologic Predictors of the Risc of Generalization in Non-Small Cell Lung Cancer Patients after Comlete Resections
Kshivets milan2014
5-YEAR SURVIVAL OF UPPER THIRD ESOPHAGEAL CANCER PATIENTS WAS SIGNIFICANTLY SUPERIOR IN COMPARISON WITH MIDDLE AND LOWER THIRD ESOPHAGEAL CANCER PATIENTS AFTER RADICAL SURGERY AND STRONGLY DEPENDED ON PHASE TRANSITION EARLY-INVASIVE CANCER, LYMPH NODE METASTASES, CELL RATIO FACTORS AND ADJUVANT CHEMOIMMUNORADIOTHERAPY
Kshivets O. Lung Cancer Surgery
NEURAL NETWORKS AND BOOTSTRAP SIMULATION IN PREDICTION OF OUTCOME OF NON-SMALL CELL LUNG CANCER PATIENTS AFTER COMPLETE LOBECTOMIES AND PNEUMONECTOMIES
Kshivets iaslc denver2021
Lung Cancer Prognosis and Cell Ratio Factors
OBJECTIVE: We examined cell ratio factors (CRF) significantly affecting non-small cell lung cancer (LC) patients (LCP) survival. CRF - ratio between cancer cells (CC) and blood cells subpopulations.
Cox modeling displayed that LCP survival significantly depended on CRF: leucocytes/CC, segmented neutrophils/CC, lymphocytes/CC, healthy cells/CC (P=0.000-0.016). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and healthy cells/CC (rank=1), segmented neutrophils/CC (rank=2), erythrocytes/CC (rank=3), thrombocytes/CC (4), leucocytes/CC (5), lymphocytes/CC (6), eosinophils/CC (7), monocytes/CC (8), stick neutrophils/CC (9). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: LCP survival after radical procedures significantly depended on CRF.
Kshivets iaslc singapore2020
Lymph Node Metastases of Lung Cancer and Blood Cell Circuit
Kshivets Oleg Surgery Department, Roshal Hospital, Moscow, Russia
OBJECTIVE: Significance of blood cell circuit in terms of detection of non-small cell lung cancer (LC) patients (LCP) with lymph node metastases was investigated.
METHODS: We analyzed data of 757 consecutive LCP (age=57.6±8.2 years; tumor size=4.1±2.4 cm) radically operated (R0) and monitored in 1985-2020 (m=654, f=103; upper lobectomies=272, lower lobectomies=176, middle lobectomies=18, bilobectomies=42, pneumonectomies=249, mediastinal lymph node dissection=757; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=192; T1=317, T2=251, T3=132, T4=57; N0=509, N1=130, N2=118, M0=757; G1=194, G2=238, G3=325; squamous=415, adenocarcinoma=292, large cell=50. Variables selected for study were input levels of blood cell circuit, sex, age, TNMG. Differences between groups were evaluated using discriminant analysis, clustering, nonlinear estimation, structural equation modeling, Monte Carlo, bootstrap simulation and neural networks computing.
RESULTS: It was revealed that separation of LCP with lymph node metastases (n=248) from LCP without metastases (n=509) significantly depended on: leucocytes (abs, total), segmented neutrophils (%, abs, total), lymphocytes (%), ESS, Rh, coagulation time, prothrombin index, fibrinogen, heparin tolerance, cell ratio factors (CRF) (ratio between cancer cells- CC and blood cells subpopulations), T, G, tumor size (P=0.047-0.000). Neural networks computing, genetic algorithm selection and bootstrap simulation revealed relationships of lymph node metastases and CRF: healthy cells/CC (rank=1), segmented neutrophils/CC (2), leucocytes/CC (3), erythrocytes/CC (4), lymphocytes/CC (5), thrombocytes/CC (6), eosinophils/CC (7), monocytes/CC (8), stick neutrophils/CC (9). Correct classification N0—N12 was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSION: Lymph node metastases significantly depended on blood cell circuit.
PRECISE EARLY DETECTION OF LUNG CANCER AND IMMUNE CIRCUIT
PRECISE EARLY DETECTION OF LUNG CANCER AND IMMUNE CIRCUIT
Kshivets wscts2015
Artificial Intelligence, System Analysis and Simulation Modeling in Precise Prediction of 5-Year Survival of Esophageal Cancer Patients after Complete Esophagogastrectomies
Kshivets aats new_york2019
Survival of Esophageal Cancer Patients was Significantly Superior in Comparison with Cardioesophageal Cancer Patients after Surgery
Kshivets Oleg Surgery Department, Roshal Hospital, Moscow, Russia
OBJECTIVE: This study aimed to determine localization influence of tumor for 5-year survival (5YS) of esophageal (EC) or cardioesophageal (CC) cancer patients (ECP, CEP) after complete en block (R0) esophagogastrectomies (EG) through left/right thoracoabdominal incision.
METHODS: We analyzed data of 543 consecutive patients (age=56.4±8.8 years; tumor size=6±3.5 cm) radically operated (R0) and monitored in 1975-2019 (m=405, f=138; ECP=259, CEP=284; esophagogastrectomies (EG) Garlock=280, EG Lewis=263, combined EG with resection of pancreas, liver, diaphragm, aorta, VCS, colon transversum, lung, trachea, pericardium, splenectomy=151; adenocarcinoma=308, squamous=225, mix=10; T1=126, T2=114, T3=178, T4=125; N0=275, N1=69, N2=199; G1=157, G2=139, G3=247; early EC=107, invasive=436; only surgery=420, adjuvant chemoimmunoradiotherapy-AT=123: 5-FU+thymalin/taktivin+radiotherapy 45-50Gy). Multivariate Cox modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 1892.4±2241 days and cumulative 5-year survival (5YS) reached 51.9%, 10 years – 45.7%, 20 years – 33.5%. 183 ECP lived more than 5 years (LS=4311±2419.7 days), 98 ECP – more than 10 years (LS=5903.4±2299.4 days). 224 died because of EC/CC (LS=629.2±320.1 days). 5YS of ECP (67.3%, LS=2605±2628.9 days) was significantly superior in comparison with CEP (36.4%, LS=1242.6±1558.5 days) (P=0.00000 by log-rank test). AT significantly improved 5YS (68.2% vs. 48.5%) (P=0.00033 by log-rank test). Cox modeling displayed that 5YS of ECP/CEP significantly depended on: phase transition (PT) N0—N12 in terms of synergetics, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), T, G, histology, age, AT, localization, blood cells, prothrombin index, coagulation time, residual nitrogen, blood group, Rh, glucose, protein (P=0.000-0.008). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and healthy cells/CC (rank=1), PT early-invasive EC (rank=2), PT N0—N12 (rank=3), erythrocytes/CC (4), thrombocytes/CC (5), stick neutrophils/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), eosinophils/CC (9), leucocytes/CC (10), monocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
Kshivets Hong Kong Sydney2020
Combined Lobectomies and Pneumonectomies: Survival Outcomes in Patients with Local Advanced Lung Cancer
Kshivets O. Esophageal & Cardioesophageal Cancer Surgery
ADJUVANT CHEMOIMMUNORADIO/CHEMOIMMUNOTHERAPY SIGNIFICANTLY IMPROVED 5-YEAR SURVIVAL OF ESOPHAGEAL/CARDIOESOPHAGEAL CANCER PATIENTS AFTER RADICAL SURGERY
Kshivets eacts milan2018
Survival Outcomes in Patients with Esophageal Cancer after Complete Esophagogastrectomies
Kshivets O. Lung Cancer Surgery
5-Year Survival of Non-Small Cell Lung Cancer Patients after Radical Surgery Significantly Depended on Phase Transition “Early-Invasive Cancer”, Lymph Node Metastases and Cell Ratio Factors
Kshivets O. Lung Cancer Stage III Surgery
PREDICTION OF 5-YEAR SURVIVAL OF NON-SMALL CELL LUNG CANCER PATIENTS WITH STAGE III AFTER COMPLETE RESECTIONS
Combined Esophagogastrectomies: Survival Outcomes in Patients with Local Adva...
CONCLUSIONS: 5YS of local advanced ECP after combined radical procedures significantly depended on: tumor characteristics, blood cell circuit, cell ratio factors, biochemical factors, hemostasis system, anthropometric data and adjuvant treatment. Optimal strategies for local advanced ECP are: 1) availability of very experienced thoracoabdominal surgeons because of complexity radical procedures; 2) aggressive en block surgery and adequate lymph node dissection for completeness; 3) precise prediction; 4) AT for ECP with unfavorable prognos
Kshivets O. Esophagogastric Cancer Surgery
ARTIFICIAL INTELLIGENCE, SYSTEM ANALYSIS AND SIMULATION MODELING IN OPTIMIZATION OF TREATMENT FOR ESOPHAGOGASTRIC CANCER PATIENTS
Lung Cancer: 10-Year Survival
CONCLUSIONS: 10-Year survival of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) anthropometric data; 10) surgery type; 11) tumor localization. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
What's hot (20)
PRECISE EARLY DETECTION OF LUNG CANCER AND IMMUNE CIRCUIT
PRECISE EARLY DETECTION OF LUNG CANCER AND IMMUNE CIRCUIT
Kshivets O. Esophageal & Cardioesophageal Cancer Surgery
Kshivets O. Esophageal & Cardioesophageal Cancer Surgery
Combined Esophagogastrectomies: Survival Outcomes in Patients with Local Adva...
Combined Esophagogastrectomies: Survival Outcomes in Patients with Local Adva...
Similar to Kshivets aats new_york2018
Esophageal Cancer: Artificial Intelligence, Synergetics, Complex System Analy...
5-year survival of ECP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC cell dynamics; 9) EC characteristics; 10) tumor localization; 11) anthropometric data; 12) surgery type. Optimal diagnosis and treatment strategies for EC are: 1) screening and early detection of EC; 2) availability of experienced thoracoabdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for ECP with unfavorable prognosis.
Kshivets Oleg Optimization of Management for Esophageal Cancer Patients (T1-...
Optimization of Management for Esophageal Cancer Patients (T1-4N0-2M0).
Kshivets Oleg Surgery Department, Bagrationovsk Hospital, Bagrationovsk, Kaliningrad, Russia
ABSTRACT
OBJECTIVE: 5-survival (5YS) and life span after radical surgery for esophageal cancer (EC) pa¬tients (ECP)(T1-4N0-2M0) - alive supersysems was analyzed. The importance must be stressed of using complex system analysis, artificial intelligence (neural networks computing), simulation modeling and statistical methods in combination, because the different approaches yield complementary pieces of prognostic information.
METHODS: We analyzed data of 563 consecutive ECP (age=56.6±8.9 years; tumor size=6±3.5 cm) radically operated (R0) and monitored in 1975-2024 (m=419, f=144; esophagogastrectomies (EG) Garlock=289, EG Lewis=274, combined EG with resection of pancreas, liver, diaphragm, aorta, VCS, colon transversum, lung, trachea, pericardium, splenectomy=170; adenocarcinoma=323, squamous=230, mix=10; T1=131, T2=119, T3=185, T4=128; N0=285, N1=71, N2=207; G1=161, G2=143, G3=259; early EC=112, invasive=451; only surgery=428, adjuvant chemoimmunoradiotherapy-AT=135: 5-FU+thymalin/taktivin+radiotherapy 45-50Gy). Multivariate Cox modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 1915.4±2284.8 days and cumulative 5-year survival (5YS) reached 52.6%, 10 years – 46.3%, 20 years – 33.3%, 30 years – 27.5%. 193 ECP lived more than 5 years (LS=4309.1±2507.4 days), 105 ECP – more than 10 years (LS=5860.8±2469.2 days). 228 ECP died because of EC (LS=629.8±324.1 days). AT significantly improved 5YS (69% vs. 49.1%) (P=0.0007 by log-rank test). 5YS of ECP of upper/3 was significantly better than others (65.3% vs.50.3%) (P=0.003). Cox modeling displayed that 5YS of ECP significantly depended on: phase transition (PT) N0—N12 in terms of synergetics, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), T, G, histology, age, AT, localization, prothrombin index, hemorrhage time, residual nitrogen, protein (P=0.000-0.019). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and healthy cells/CC (rank=1), PT N0—N12 (2), PT early-invasive EC (3), erythrocytes/CC (4), thrombocytes/CC (5); segmented neutrophils/CC (6), stick neutrophils/CC (7), lymphocytes/CC (8), eosinophils/CC (9), monocytes/CC (10), leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5-year survival of ECP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC cell dynamics; 9) EC characteristics; 10) tumor localization; 11) anthropometric data; 12) surgery type. Optimal diagnosis and trea
Local Advanced Esophageal Cancer (T3-4N0-2M0): Artificial Intelligence, Syner...
5YS of local advanced ECP after combined radical procedures significantly depended on: tumor characteristics, blood cell circuit, cell ratio factors, biochemical factors, hemostasis system, anthropometric data and adjuvant treatment. Optimal strategies for local advanced ECP are: 1) availability of very experienced thoracoabdominal surgeons because of complexity radical procedures; 2) aggressive en block surgery and adequate lymph node dissection for completeness; 3) precise prediction; 4) AT for ECP with unfavorable prognosis.
Lung Cancer: Precise Prediction
OBJECTIVE: 5-survival (5YS) and life span after radical surgery for non-small cell lung cancer (LC) pa¬tients (LCP) (T1-4N0-2M0) was analyzed.
METHODS: We analyzed data of 771 consecutive LCP (age=57.6±8.3 years; tumor size=4.1±2.4 cm) radically operated and monitored in 1985-2022 (m=662, f=109; upper lobectomies=278, lower lobectomies=178, middle lobectomies=18, bilobectomies=42, pneumonectomies=255, mediastinal lymph node dissection=771; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=194; only surgery-S=620, adjuvant chemoimmunoradiotherapy-AT=151: CAV/gemzar + cisplatin + thymalin/taktivin + radiotherapy 45-50Gy; T1=322, T2=255, T3=133, T4=61; N0=518, N1=131, N2=122, M0=771; G1=195, G2=243, G3=333; squamous=418, adenocarcinoma=303, large cell=50; early LC=215, invasive LC=556; right LC=413, left LC=358; central=291; peripheral=480. Variables selected for study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Regression modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine significant dependence.
RESULTS: Overall life span (LS) was 2240.9±1748.8 days and cumulative 5-year survival (5YS) reached 73%, 10 years – 64.2%, 20 years – 43%. 503 LCP lived more than 5 years (LS=3126.6±1536 days), 145 LCP – more than 10 years (LS=5068.5±1513.2 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (77.7% vs.63.4%, P=0.00001 by log-rank test). AT significantly improved 5YS (64.4% vs. 34.8%) (P=0.00003 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.035). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), eosinophils/CC (4), erythrocytes/CC (5),healthy cells/CC (6), segmented neutrophils/CC (7), lymphocytes/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data.
Kshivets_ELCC2023.pdf
OBJECTIVE: 5-survival (5YS) and life span after radical surgery for non-small cell lung cancer (LC) pa¬tients (LCP) (T1-4N0-2M0) was analyzed.
METHODS: We analyzed data of 771 consecutive LCP (age=57.6±8.3 years; tumor size=4.1±2.4 cm) radically operated and monitored in 1985-2022 (m=662, f=109; upper lobectomies=278, lower lobectomies=178, middle lobectomies=18, bilobectomies=42, pneumonectomies=255, mediastinal lymph node dissection=771; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=194; only surgery-S=620, adjuvant chemoimmunoradiotherapy-AT=151: CAV/gemzar + cisplatin + thymalin/taktivin + radiotherapy 45-50Gy; T1=322, T2=255, T3=133, T4=61; N0=518, N1=131, N2=122, M0=771; G1=195, G2=243, G3=333; squamous=418, adenocarcinoma=303, large cell=50; early LC=215, invasive LC=556; right LC=413, left LC=358; central=291; peripheral=480. Variables selected for study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Regression modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine significant dependence.
RESULTS: Overall life span (LS) was 2240.9±1748.8 days and cumulative 5-year survival (5YS) reached 73%, 10 years – 64.2%, 20 years – 43%. 503 LCP lived more than 5 years (LS=3126.6±1536 days), 145 LCP – more than 10 years (LS=5068.5±1513.2 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (77.7% vs.63.4%, P=0.00001 by log-rank test). AT significantly improved 5YS (64.4% vs. 34.8%) (P=0.00003 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.035). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), eosinophils/CC (4), erythrocytes/CC (5),healthy cells/CC (6), segmented neutrophils/CC (7), lymphocytes/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data.
Kshivets_ELCC2023.pdf
OBJECTIVE: 5-survival (5YS) and life span after radical surgery for non-small cell lung cancer (LC) pa¬tients (LCP) (T1-4N0-2M0) was analyzed.
METHODS: We analyzed data of 771 consecutive LCP (age=57.6±8.3 years; tumor size=4.1±2.4 cm) radically operated and monitored in 1985-2022 (m=662, f=109; upper lobectomies=278, lower lobectomies=178, middle lobectomies=18, bilobectomies=42, pneumonectomies=255, mediastinal lymph node dissection=771; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=194; only surgery-S=620, adjuvant chemoimmunoradiotherapy-AT=151: CAV/gemzar + cisplatin + thymalin/taktivin + radiotherapy 45-50Gy; T1=322, T2=255, T3=133, T4=61; N0=518, N1=131, N2=122, M0=771; G1=195, G2=243, G3=333; squamous=418, adenocarcinoma=303, large cell=50; early LC=215, invasive LC=556; right LC=413, left LC=358; central=291; peripheral=480. Variables selected for study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Regression modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine significant dependence.
RESULTS: Overall life span (LS) was 2240.9±1748.8 days and cumulative 5-year survival (5YS) reached 73%, 10 years – 64.2%, 20 years – 43%. 503 LCP lived more than 5 years (LS=3126.6±1536 days), 145 LCP – more than 10 years (LS=5068.5±1513.2 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (77.7% vs.63.4%, P=0.00001 by log-rank test). AT significantly improved 5YS (64.4% vs. 34.8%) (P=0.00003 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.035). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), eosinophils/CC (4), erythrocytes/CC (5),healthy cells/CC (6), segmented neutrophils/CC (7), lymphocytes/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: PT early-invasive cancer; PT N0--N12; cell ratio factors; blood cell circuit; biochemical factors; hemostasis system; AT; LC characteristics; surgery type; anthropometric data.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Transplanting cardiac amyloidosis when to refer for heart transplant
Transplanting cardiac amyloidosis when to refer for heart transplant
Kshivets O. Cardioesophageal Cancer Surgery
ARTFICIAL INTELLIGENCE, SYSTEM ANALYSIS AND SIMULATION MODELING IN PREDICTION OF
5-YEAR SURVIVAL OF CARDIOESOPHAGEAL CANCER PATIENTS AFTER COMPLETE LEFT THORACOABDOMINAL ESOPHAGOGASTRECTOMIES
Kshivets esmo2021
Esophageal cancer cell dynamics significantly depended on blood cell circuit, biochemical factors, hemostasis system, cancer characteristics, anthropometric data.
Kshivets chicago2016
Artificial Intelligence, System Analysis and Simulation Modeling in Optimization of Management for Lung Cancer Patients
Kshivets O. Esophageal Cancer Surgery
ARTFICIAL INTELLIGENCE, SYSTEM ANALYSIS AND SIMULATION MODELING IN OPTIMIZATION OF TREATMENT FOR ESOPHAGEAL CANCER PATIENTS AFTER COMPLETE ESOPHAGECTOMIES
Kshivets elcc2022
It was revealed that separation of LCP with early LC (n=215) from invasive LCP (n=555) significantly depended on: Hb, leucocytes (abs, total), thrombocytes (abs, tot), erythrocytes (abs, tot), segmented neutrophils (%, abs, total), stick neutrophils (%, abs, total), lymphocytes (%), monocytes (abs, tot), ESS, coagulation time, fibrinogen, cell ratio factors (CRF) (ratio between cancer cells- CC and blood cells subpopulations), tumor size, age, tumor growth, T1-4, G1-3, PT N0---N12 (P=0.046-0.000). Neural networks computing, genetic algorithm selection and bootstrap simulation revealed relationships of PT early—invasive cancer and CRF: healthy cells/CC (rank=1), erythrocytes/CC (2), stick neutrophils/CC (3), thrombocytes/CC (4), eosinophils/CC (5), segmented neutrophils/CC (6), lymphocytes/CC (7), monocytes/CC (8), leucocytes/CC (9). Correct classification PT early—invasive cancer was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSION: Blood cell circuit significantly influenced the phase transition early—invasive lung cancer.
Stem cells therapy for peripheral arterial occlusive disease
Stem cells therapy for peripheral arterial occlusive disease
Similar to Kshivets aats new_york2018 (18)
Esophageal Cancer: Artificial Intelligence, Synergetics, Complex System Analy...
Esophageal Cancer: Artificial Intelligence, Synergetics, Complex System Analy...
Kshivets Oleg Optimization of Management for Esophageal Cancer Patients (T1-...
Kshivets Oleg Optimization of Management for Esophageal Cancer Patients (T1-...
Local Advanced Esophageal Cancer (T3-4N0-2M0): Artificial Intelligence, Syner...
Local Advanced Esophageal Cancer (T3-4N0-2M0): Artificial Intelligence, Syner...
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...
Transplanting cardiac amyloidosis when to refer for heart transplant
Transplanting cardiac amyloidosis when to refer for heart transplant
Stem cells therapy for peripheral arterial occlusive disease
Stem cells therapy for peripheral arterial occlusive disease
More from Oleg Kshivets
Gastric Cancer: Сlinical Implementation of Artificial Intelligence, Synergeti...
5-year survival of GCP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) GC cell dynamics; 9) GC characteristics; 10) tumor localization; 11) anthropometric data; 12) surgery type. Optimal diagnosis and treatment strategies for GC are: 1) screening and early detection of GC; 2) availability of sufficient quantity of experienced abdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunotherapy for GCP with unfavorable prognosis.
Kshivets_IASLC_Singapore2023.pdf
5YS of LCP after radical procedures significantly depended on: PT early-invasive cancer; PT N0--N12; cell ratio factors; blood cell circuit; biochemical factors; hemostasis system; AT; LC characteristics; LC cell dynamics; surgery type; anthropometric data.
KshivetsWSCTS2023_Brazil.pdf
5-year survival of ECP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC characteristics; 9) EC cell dynamics; 10) tumor localization; 11) anthropometric data; 12) surgery type. Optimal diagnosis and treatment strategies for EC are: 1) screening and early detection of EC; 2) availability of experienced thoracoabdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for ECP with unfavorable prognosis.
KshivetsWSCTS2023_Brazil.pdf
OBJECTIVE: 5-survival (5YS) and life span after radical surgery for esophageal cancer (EC) pa¬tients (ECP) (T1-4N0-2M0) was analyzed. The importance must be stressed of using complex system analysis, artificial intelligence (neural networks computing), simulation modeling and statistical methods in combination, because the different approaches yield complementary pieces of prognostic information.
METHODS: We analyzed data of 557 consecutive ECP (age=56.6±8.9 years; tumor size=6±3.5 cm) radically operated (R0) and monitored in 1975-2023 (m=415, f=142; esophagogastrectomies (EG) Garlock=288, EG Lewis=269, combined EG with resection of pancreas, liver, diaphragm, aorta, VCS, colon transversum, lung, trachea, pericardium, splenectomy=168; adenocarcinoma=319, squamous=228, mix=10; T1=130, T2=115, T3=184, T4=128; N0=282, N1=70, N2=205; G1=157, G2=142, G3=258; early EC=111, invasive=446; only surgery=425, adjuvant chemoimmunoradiotherapy-AT=132: 5-FU+thymalin/taktivin+radiotherapy 45-50Gy). Multivariate Cox modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 1876.9±2219.8 days and cumulative 5-year survival (5YS) reached 52%, 10 years – 45.5%, 20 years – 33.4%, 30 years – 26.9%. 187 ECP lived more than 5 years (LS=4271±2411.9 days), 99 ECP – more than 10 years (LS=5883±2296.6 days). 228 ECP died because of EC (LS=629.8±324.1 days). AT significantly improved 5YS (67.8% vs. 48.7%) (P=0.00084 by log-rank test). Cox modeling displayed that 5YS of ECP significantly depended on: phase transition (PT) N0—N12 in terms of synergetics, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), T, G, histology, age, AT, localization, prothrombin index, hemorrhage time, residual nitrogen, protein (P=0.000-0.019). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and
healthy cells/CC (rank=1), PT early-invasive EC (2); PT N0—N12 (3), erythrocytes/CC (4), thrombocytes/CC (5); stick neutrophils/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), eosinophils/CC (9), leucocytes/CC (10); monocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5-year survival of ECP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC characteristics; 9) EC cell dynamics; 10) tumor localization; 11) anthropometric data; 12) surgery type. Optimal diagnosis and treatment strategies for EC are: 1) screening and early detection of EC; 2) availability of experienced thoracoabdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5)AT
KshivetsWSCTS2023_Brazil.pdf
OBJECTIVE: 5-survival (5YS) and life span after radical surgery for esophageal cancer (EC) pa¬tients (ECP) (T1-4N0-2M0) was analyzed. The importance must be stressed of using complex system analysis, artificial intelligence (neural networks computing), simulation modeling and statistical methods in combination, because the different approaches yield complementary pieces of prognostic information.
METHODS: We analyzed data of 557 consecutive ECP (age=56.6±8.9 years; tumor size=6±3.5 cm) radically operated (R0) and monitored in 1975-2023 (m=415, f=142; esophagogastrectomies (EG) Garlock=288, EG Lewis=269, combined EG with resection of pancreas, liver, diaphragm, aorta, VCS, colon transversum, lung, trachea, pericardium, splenectomy=168; adenocarcinoma=319, squamous=228, mix=10; T1=130, T2=115, T3=184, T4=128; N0=282, N1=70, N2=205; G1=157, G2=142, G3=258; early EC=111, invasive=446; only surgery=425, adjuvant chemoimmunoradiotherapy-AT=132: 5-FU+thymalin/taktivin+radiotherapy 45-50Gy). Multivariate Cox modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 1876.9±2219.8 days and cumulative 5-year survival (5YS) reached 52%, 10 years – 45.5%, 20 years – 33.4%, 30 years – 26.9%. 187 ECP lived more than 5 years (LS=4271±2411.9 days), 99 ECP – more than 10 years (LS=5883±2296.6 days). 228 ECP died because of EC (LS=629.8±324.1 days). AT significantly improved 5YS (67.8% vs. 48.7%) (P=0.00084 by log-rank test). Cox modeling displayed that 5YS of ECP significantly depended on: phase transition (PT) N0—N12 in terms of synergetics, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), T, G, histology, age, AT, localization, prothrombin index, hemorrhage time, residual nitrogen, protein (P=0.000-0.019). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and
healthy cells/CC (rank=1), PT early-invasive EC (2); PT N0—N12 (3), erythrocytes/CC (4), thrombocytes/CC (5); stick neutrophils/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), eosinophils/CC (9), leucocytes/CC (10); monocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5-year survival of ECP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC characteristics; 9) EC cell dynamics; 10) tumor localization; 11) anthropometric data; 12) surgery type. Optimal diagnosis and treatment strategies for EC are: 1) screening and early detection of EC; 2) availability of experienced thoracoabdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant ch
Kshivets_WCGIC2023.pdf
5-year survival of GCP after radical procedures
significantly depended on: 1) PT “early-invasive
cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood
cell circuit; 5) biochemical factors; 6) hemostasis
system; 7) AT; 8) GC characteristics; 9) GC cell
dynamics; 10) tumor localization; 11) anthropometric
data; 12) surgery type. Best diagnosis and treatment
strategies for GC are: 1) screening and early detection
of GC; 2) availability of experienced abdominal
surgeons because of complexity of radical procedures;
3) aggressive en block surgery and adequate lymph
node dissection for completeness; 4) precise
prediction; 5) adjuvant chemoimmunotherapy for GCP
with unfavorable prognosis.
Kshivets_SPB_WSCTS2022Lung.pdf
Survival of Lung Cancer Patients after Lobectomies was Significantly Superior in Comparison with Lung Cancer Patients after Pneumonectomies
Lung cancer cell dynamics significantly depended on blood cell circuit, bioch...
OBJECTIVE: We examined factors significantly affecting lung cancer (LC) cell dynamics.
METHODS: We analyzed data of 768 consecutive non-small cell LC patients (LCP) (age=57.6±8.3 years; tumor size=4.1±2.4 cm) radically operated and monitored in 1985-2022 (m=660, f=108; upper lobectomies=277, lower lobectomies=177, middle lobectomies=18, bilobectomies=42, pneumonectomies=254, mediastinal lymph node dissection=768; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=193; only surgery-S=618, adjuvant chemoimmunoradiotherapy-AT=150: CAV/gemzar + cisplatin + thymalin/taktivin + radiotherapy 45-50Gy; T1=320, T2=255, T3=133, T4=60; N0=516, N1=131, N2=121, M0=768; G1=194, G2=243, G3=331; squamous=417, adenocarcinoma=301, large cell=50; early LC=214, invasive LC=554; right LC=412, left LC=356; central=290; peripheral=478. Variables selected for study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Regression modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine significant dependence.
RESULTS: Overall life span (LS) was 2244.9±1750.3 days and cumulative 5-year survival (5YS) reached 72.9%, 10 years – 64.3%, 20 years – 43.1%. 502 LCP lived more than 5 years (LS=3128.7±1536.8 days), 145 LCP – more than 10 years (LS=5068.5±1513.2 days).199 LCP died because of LC (LS=562.7±374.5 days). Regression modeling displayed LC cell dynamics significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, histology, T, G, LC growth, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), ESS, glucose, bilirubin (P=0.000-0.033). Neural networks simulation revealed relationships between LC cell dynamics and segmented neutrophils (rank=1), lymphocytes (2), PT N0—N12 (3), PT early-invasive LC (4), leucocytes (5), stick neutrophils (6), eosinophils (7), erythrocytes (8), monocytes (9), thrombocytes (10), Hb (11), ESS (12). Prediction was 92-95% by neural networks computing.
CONCLUSIONS: Lung cancer cell dynamics significantly depended on blood cell circuit, biochemical factors, hemostasis system, cancer characteristics, anthropometric data.
Esophageal Cancer: Precise Prediction
OBJECTIVE: 5-survival (5YS) and life span after radical surgery for esophageal cancer (EC) pa¬tients (ECP) (T1-4N0-2M0) was analyzed.
METHODS: We analyzed data of 556 consecutive ECP (age=56.5±8.9 years; tumor size=6±3.5 cm) radically operated (R0) and monitored in 1975-2022 (m=415, f=141; esophagogastrectomies (EG) Garlock=287, EG Lewis=269, combined EG with resection of pancreas, liver, diaphragm, aorta, VCS, colon transversum, lung, trachea, pericardium, splenectomy=167; adenocarcinoma=318, squamous=228, mix=10; T1=129, T2=115, T3=184, T4=128; N0=281, N1=70, N2=205; G1=157, G2=141, G3=258; early EC=110, invasive=446; only surgery=424, adjuvant chemoimmunoradiotherapy-AT=132: 5-FU+thymalin/taktivin+radiotherapy 45-50Gy). Multivariate Cox modeling, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 1877±2221.6 days and cumulative 5-year survival (5YS) reached 52%, 10 years – 45%, 20 years – 33.4%, 30 years – 27%. 186 ECP lived more than 5 years (LS=4283.3±2412.6 days), 99 ECP – more than 10 years (LS=5883±2296.6 days). 227 ECP died because of EC (LS=631.8±323.4 days). AT significantly improved 5YS (60.3% vs. 42%) (P=0.0029 by log-rank test). Cox modeling displayed that 5YS of ECP significantly depended on: phase transition (PT) N0—N12 in terms of synergetics, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), T, G, histology, age, AT, localization, prothrombin index, hemorrhage time, residual nitrogen, protein (P=0.000-0.021). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and P PT early-invasive EC (rank=1); healthy cells/CC (2), erythrocytes/CC (3), PT N0—N12 (4) thrombocytes/CC (5); segmented neutrophils/CC (6), stick neutrophils/CC (7), lymphocytes/CC (8), monocytes/CC (9); leucocytes/CC (10); eosinophils/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5-year survival of ECP after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC characteristics; 9) tumor localization; 10) anthropometric data; 11) surgery type. Optimal diagnosis and treatment strategies for EC are: 1) screening and early detection of EC; 2) availability of experienced thoracoabdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for ECP with unfavorable prognosis.
Survival of Lung Cancer Patients after Lobectomies was Significantly Superior...
OBJECTIVE: This study aimed to determine surgery type influence for 5-year survival (5YS) of non-small cell lung cancer (LC) patients (LCP) after complete en block (R0) lobectomies and pneumonectomies.
METHODS: We analyzed data of 765 consecutive patients (age=57.6±8.3 years; tumor size=4.1±2.4 cm) radically operated (R0) and monitored in 1985-2022 (m=659, f=106; bi/lobectomies=512, pneumonectomies=253, mediastinal lymph node dissection=765; combined procedures with resection of trachea, carina, atrium, aorta, VCS, vena azygos, pericardium, liver, diaphragm, ribs, esophagus=192; only surgery-S=616, adjuvant chemoimmunoradiotherapy-AT=149: CAV/gemzar + cisplatin + thymalin/taktivin + radiotherapy 45-50Gy; T1=318, T2=255, T3=133, T4=59; N0=514, N1=131, N2=120, M0=765; G1=194, G2=241, G3=330; squamous=417, adenocarcinoma=298, large cell=50; early LC=212, invasive LC=553. Multivariate Cox modeling, discriminant analysis, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 2240.1±1751.6 days and cumulative 5-year survival (5YS) reached 72.8%, 10 years – 64.2%, 20 years – 42.9%. 499 LCP lived more than 5 years (LS=3126.8±1540 days), 143 LCP – more than 10 years (LS=5083.3±1518.6 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (77.6% vs.63.1%, P=0.00001 by log-rank test). AT significantly improved 5YS (64.4% vs. 34.8%) (P=0.00003 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). 5YS of LCP after Lobectomies (77.6%) was significantly superior in comparison with LCP after pneumonectomies (63%) (P=0.00001 by log-rank test). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12(rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), segmented neutrophils/CC (7), lymphocytes/CC (8), monocytes/CC (9); stick neutrophils/CC (10), leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) surgery type: lobectomy/pneumonectomy; 10) anthropometric data.
• Gastric cancer prognosis and cell ratio factors
OBJECTIVE: We examined cell ratio factors (CRF) significantly affecting gastric cancer (EC) patients GCP) survival. CRF - ratio between cancer cells (CC) and blood cells subpopulations.
METHODS: We analyzed data of 799 consecutive GCP (T1-4N0-2M0) (age=57.1±9.4 years; tumor size=5.4±3.1 cm) radically operated (R0) and monitored in 1975-2022 (m=558, f=241; total gastrectomies=173, distal gastrectomies=461; proximal gastrectomies=165; combined gastrectomies=247 with resection of esophagus, pancreas, liver, duodenum, diaphragm, colon transversum, splenectomy, etc; only surgery-S=624, adjuvant chemoimmunotherapy-AT=175 (5-FU + thymalin/taktivin); T1=238, T2=220, T3=184, T4=157; N0=437, N1=109, N2=253, M0=799; G1=222, G2=164, G3=413. Variables selected for prognosis study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Survival curves were estimated by the Kaplan-Meier method. Differences in curves between groups of GCP were evaluated using a log-rank test. Multivariate Cox modeling, discriminant analysis, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence.
RESULTS: Overall life span (LS) was 2128.9±2300.3 days and cumulative 5-year survival (5YS) reached 58.4%, 10 years – 51.9%, 20 years – 39%, 30 years – 27.2%. 318 GCP lived more than 5 years (LS=4304.5±2290.6 days), 169 GCP – more than 10 years (LS=5919.5±2020 days). 290 GCP died because of GC (LS=651±347.2 days). Cox modeling displayed that G CP survival significantly depended on CRF: healthy cells/CC, erythrocytes/CC, monocytes/CC, phase transition (PT) in terms of synergetics early—invasive cancer; PT N0--N12, age, G1-3, hemorrhage time, ESS, sex, AT, prothrombin index, residual nitrogen. Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early—invasive cancer (rank=1); PT N0--N12 (2); healthy cells/CC (3), erythrocytes/CC (4), thrombocytes/CC (5), monocytes/CC (6), segmented neutrophils/CC (7), leucocytes/CC (8), lymphocytes/CC (9), stick neutrophils/CC (10), eosinophils/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: GCP survival after radical procedures significantly depended on CRF.
Kshivets gc 10_ys_wjarr-2021-0659
10-Year survival of GCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) GC characteristics; 9) anthropometric data; 10) surgery type. Optimal diagnosis and treatment strategies for GC are: 1) screening and early detection of GC; 2) availability of experienced abdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunotherapy for GCP with unfavorable prognosis.
Kshivets lc10 ys_wjarr
Conclusions: 10-Year survival of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) anthropometric data; 10) surgery type. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Kshivets eso10 y2021
10-Year survival after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC characteristics; 9) tumor localization; 10) anthropometric data; 11) surgery type. Optimal diagnosis and treatment strategies for EC are: 1) screening and early detection of EC; 2) availability of experienced thoracoabdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for ECP with unfavorable prognosis.
Kshivets ny2021aats
CONCLUSIONS: 10-Year survival after radical procedures significantly depended on: 1) PT “early-invasive cancer”; 2) PT N0--N12; 3) Cell Ratio Factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) EC characteristics; 9) tumor localization; 10) anthropometric data; 11) surgery type. Optimal diagnosis and treatment strategies for EC are: 1) screening and early detection of EC; 2) availability of experienced thoracoabdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for ECP with unfavorable prognosis.
2021 esmo world_gi_poster_kshivets
Gastric Cancer: 10-Year Survival
Kshivets Oleg Surgery Department, Roshal Hospital, Moscow, Russia
CONCLUSIONS: 10-Year survival of GCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) GC characteristics; 9) anthropometric data; 10) surgery type. Optimal diagnosis and treatment strategies for GC are: 1) screening and early detection of GC; 2) availability of experienced abdominal surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunotherapy for GCP with unfavorable prognosis.
More from Oleg Kshivets (17)
Gastric Cancer: Сlinical Implementation of Artificial Intelligence, Synergeti...
Gastric Cancer: Сlinical Implementation of Artificial Intelligence, Synergeti...
Lung cancer cell dynamics significantly depended on blood cell circuit, bioch...
Lung cancer cell dynamics significantly depended on blood cell circuit, bioch...
Survival of Lung Cancer Patients after Lobectomies was Significantly Superior...
Survival of Lung Cancer Patients after Lobectomies was Significantly Superior...
Recently uploaded
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journey
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
micro teaching on communication m.sc nursing.pdf
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
Novas diretrizes da OMS para os cuidados perinatais de mais qualidade
Novas diretrizes da OMS para os cuidados perinatais de mais qualidadeProf. Marcus Renato de Carvalho
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
Prix Galien International 2024 Forum Program
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Couples presenting to the infertility clinic- Do they really have infertility...
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Physiology of Chemical Sensation of smell.pdf
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
ANATOMY AND PHYSIOLOGY OF URINARY SYSTEM.pptx
Valuable Content of Human Anatomy and Physiology of Urinary system as per PCI Syllabus for Pharmacy and PharmD Students.
Charaka Samhita Sutra sthana Chapter 15 Upakalpaniyaadhyaya
Charaka Samhita Sutra sthana Chapter 15 Upakalpaniyaadhyaya
Hemodialysis: Chapter 3, Dialysis Water Unit - Dr.Gawad
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Knee anatomy and clinical tests 2024.pdf
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
New Drug Discovery and Development .....
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
Ocular injury ppt Upendra pal optometrist upums saifai etawah
This ppt are composed by upendra pal to provide help future optometrist of india
Recently uploaded (20)
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journey
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journey
Novas diretrizes da OMS para os cuidados perinatais de mais qualidade
Novas diretrizes da OMS para os cuidados perinatais de mais qualidade
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?
Couples presenting to the infertility clinic- Do they really have infertility...
Couples presenting to the infertility clinic- Do they really have infertility...
Pharynx and Clinical Correlations BY Dr.Rabia Inam Gandapore.pptx
Pharynx and Clinical Correlations BY Dr.Rabia Inam Gandapore.pptx
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...
Charaka Samhita Sutra sthana Chapter 15 Upakalpaniyaadhyaya
Charaka Samhita Sutra sthana Chapter 15 Upakalpaniyaadhyaya
Hemodialysis: Chapter 3, Dialysis Water Unit - Dr.Gawad
Hemodialysis: Chapter 3, Dialysis Water Unit - Dr.Gawad
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Surat @ℂall @Girls ꧁❤8527049040❤꧂@ℂall @Girls Service Vip Top Model Safe
Triangles of Neck and Clinical Correlation by Dr. RIG.pptx
Triangles of Neck and Clinical Correlation by Dr. RIG.pptx
Ocular injury ppt Upendra pal optometrist upums saifai etawah
Ocular injury ppt Upendra pal optometrist upums saifai etawah
Kshivets aats new_york2018
- 1. Precise Early Detection of Esophageal Cancer and Blood Cell Circuit P25 Oleg Kshivets, MD, PhD Surgery Department, Roshal Hospital, Roshal, Moscow, Russia Objective: Significance of blood cell circuit in terms of early detection of esophageal cancer (EC) was investigated. Methods: In trial (1975-2018) consecutive cases after surgery, monitored 82 EC patients (ECP) (m=60, f=22; esophagectomies Lewis=70, esophagectomies Garlock=12) with pathologic stage IA (tumor size=1.46±0.48 cm; squamous=48, adenocarcinoma=34; T1N0M0=82; G1=46, G2=22, G3=14, 5-year survival=100%) and 120 healthy donors (HD) (m=69, f=51) were reviewed. Variables selected for study were input levels of blood cell circuit, sex, age, TNMG. Differences between groups were evaluated using discriminant analysis, clustering, nonlinear estimation, structural equation modeling, Monte Carlo, bootstrap simulation and neural networks computing. Results: It was revealed that early detection of EC from HD (n=202) significantly depended on: leucocytes (abs, total), segmented neutrophils (%, abs, total), lymphocytes (%, abs), monocytes (%, abs, total), stick neutrophils (%, abs, total), eosinophils (%, abs, total) (P=0.048-0.000). Neural networks computing, genetic algorithm selection and bootstrap simulation revealed relationships of early detection of EC and lymphocytes (rank=1), segmented neutrophils (rank=2), monocytes (3), leucocytes (4), eosinophils (5), stick neutrophils (6). Correct detection of early ECP was 100% by neural networks computing (error=0.000; area under ROC curve=1.0). Conclusion: Early detection of EC from HD significantly depended on blood cell circuit. Neural Networks: n=202; Baseline Error=0.000; Area under ROC Curve=1.000; Correct Classification Rate=100% Rank Sensitivity Lymphocytes Segmented Neutrophils Monocyte Leucocytes Eosinophils Stick Neutrophils 1 2 3 4 5 8 1270 569 387 364 263 247 Blood Factors Mean Norm Mean EC t-value p Std.Dev. Norm Std.Dev. EC Leucocytes 4.96500 6.01463 -4.28094 0.000029 1.58240 1.88471 Stick Neutrophils 1.05833 1.50000 -2.12950 0.034436 1.32396 1.61207 Segmented Neutrophils 55.85833 65.69512 -6.00144 0.000000 10.68990 12.46000 Eosinophils 3.22500 1.81707 3.23342 0.001431 3.66556 1.75068 Monocytes 3.11667 4.86585 -4.86415 0.000002 2.38406 2.68403 Lymphocytes 36.82500 25.93902 7.11851 0.000000 10.32714 11.16249 Eosinophils (abs) 0.16319 0.10306 2.18615 0.029965 0.23783 0.08879 Stick Neutrophils (abs) 0.05908 0.09315 -2.58157 0.010550 0.08058 0.10682 Segmented Neutrophils (abs) 2.81104 3.97573 -6.07321 0.000000 1.17819 1.54411 Lymphocytes (abs) 1.78054 1.53635 2.28731 0.023224 0.68395 0.82678 Monocytes (abs) 0.15323 0.29521 -6.23906 0.000000 0.13311 0.19041 Eosinophils (tot) 0.78646 0.51523 1.98565 0.048438 1.17369 0.46953 Stick Neutrophils (tot) 0.28479 0.48383 -2.90713 0.004059 0.40818 0.56480 Segmented Neutrophils (tot) 13.48591 20.04112 -6.25576 0.000000 6.00216 8.89620 Monocytes (tot) 0.73147 1.46806 -6.21523 0.000000 0.65846 1.02587 Leucocytes (tot) 23.80685 30.19826 -4.64835 0.000006 8.30366 11.22937 N=202 Model: Logistic regression (logit) N of 0's: 120 1's: 82 Dep. var: NORM--CA Loss: Max likelihood Final loss: 85.816840002 Chi2( 17)=101.21 p=.00000 Modeled probability that P = norm Const.B0 L ST S E M LYM Eabs STabs Sabs LYMabs Mabs Etot STtot Stot LYMtot Mtot Ltot Estimate 319.565 45.26 -2.6078 -3.1686 -3.0135 -2.8227 -3.375 -70.14 -67.19 -46.40 -40.72 -43.43 20 19 17 16 16 -16.6368 Odds ratio (unit ch) 0.0737 0.04206 0.0491 0.05944 0.034 0.000 0.000 0.000 0.000 0.000 581987200 127613700 21046710 9372915 11601350 0.0000 Odds ratio (range) 0.0000 0.00000 0.0000 0.00000 0.000 0.000 0.000 0.000 0.000 0.000 0.0000 Bootstrap Simulation Significant Factors (Number of Samples=3333) Rank Kendall’Tau-A P< Lymphocytes 1 0.272 0.001 Monocytes tot 2 -0.234 0.001 Monocytes abs 3 -0.230 0.001 Segmented Neutrophils 4 -0.225 0.001 Segmented Neutrophils tot 5 -0.222 0.001 Segmented Neutrophils abs 6 -0.219 0.001 Monocytes 7 -0.195 0.001 Leucocytes tot 8 -0.159 0.01 Leucocytes 9 -0.155 0.01 Eosinophils 10 0.143 0.01 Lymphocytes abs 11 0.112 0.05