• Gastric cancer prognosis and cell ratio factors

OBJECTIVE: We examined cell ratio factors (CRF) significantly affecting gastric cancer (EC) patients GCP) survival. CRF - ratio between cancer cells (CC) and blood cells subpopulations. METHODS: We analyzed data of 799 consecutive GCP (T1-4N0-2M0) (age=57.1±9.4 years; tumor size=5.4±3.1 cm) radically operated (R0) and monitored in 1975-2022 (m=558, f=241; total gastrectomies=173, distal gastrectomies=461; proximal gastrectomies=165; combined gastrectomies=247 with resection of esophagus, pancreas, liver, duodenum, diaphragm, colon transversum, splenectomy, etc; only surgery-S=624, adjuvant chemoimmunotherapy-AT=175 (5-FU + thymalin/taktivin); T1=238, T2=220, T3=184, T4=157; N0=437, N1=109, N2=253, M0=799; G1=222, G2=164, G3=413. Variables selected for prognosis study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Survival curves were estimated by the Kaplan-Meier method. Differences in curves between groups of GCP were evaluated using a log-rank test. Multivariate Cox modeling, discriminant analysis, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence. RESULTS: Overall life span (LS) was 2128.9±2300.3 days and cumulative 5-year survival (5YS) reached 58.4%, 10 years – 51.9%, 20 years – 39%, 30 years – 27.2%. 318 GCP lived more than 5 years (LS=4304.5±2290.6 days), 169 GCP – more than 10 years (LS=5919.5±2020 days). 290 GCP died because of GC (LS=651±347.2 days). Cox modeling displayed that G CP survival significantly depended on CRF: healthy cells/CC, erythrocytes/CC, monocytes/CC, phase transition (PT) in terms of synergetics early—invasive cancer; PT N0--N12, age, G1-3, hemorrhage time, ESS, sex, AT, prothrombin index, residual nitrogen. Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early—invasive cancer (rank=1); PT N0--N12 (2); healthy cells/CC (3), erythrocytes/CC (4), thrombocytes/CC (5), monocytes/CC (6), segmented neutrophils/CC (7), leucocytes/CC (8), lymphocytes/CC (9), stick neutrophils/CC (10), eosinophils/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0). CONCLUSIONS: GCP survival after radical procedures significantly depended on CRF.
Recommended

Recommended
More Related Content
Similar to • Gastric cancer prognosis and cell ratio factors
Similar to • Gastric cancer prognosis and cell ratio factors (20)
More from Oleg Kshivets
More from Oleg Kshivets (15)
Recently uploaded
Recently uploaded (20)
• Gastric cancer prognosis and cell ratio factors
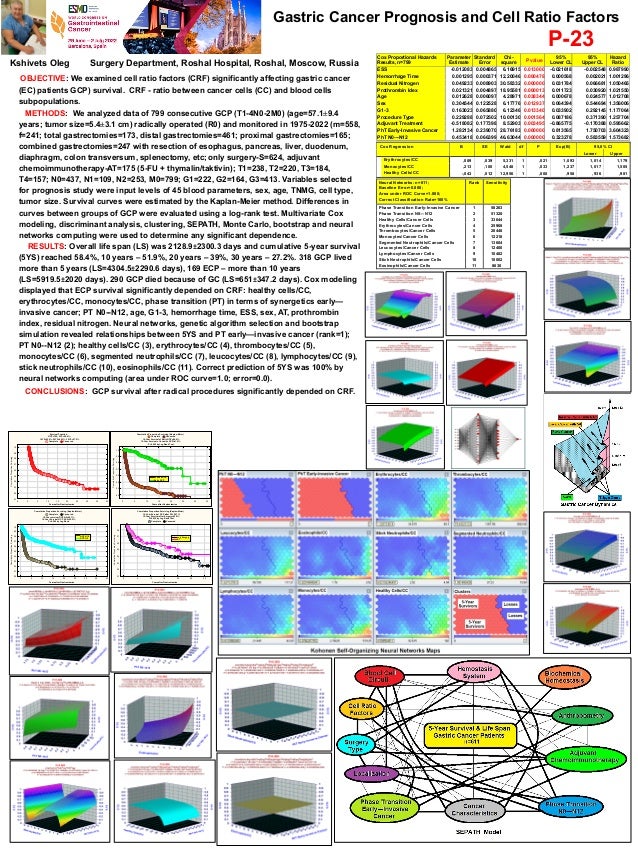
- 1. Gastric Cancer Prognosis and Cell Ratio Factors Kshivets Oleg Surgery Department, Roshal Hospital, Roshal, Moscow, Russia P-23 OBJECTIVE: We examined cell ratio factors (CRF) significantly affecting gastric cancer (EC) patients GCP) survival. CRF - ratio between cancer cells (CC) and blood cells subpopulations. METHODS: We analyzed data of 799 consecutive GCP (T1-4N0-2M0) (age=57.1±9.4 years; tumor size=5.4±3.1 cm) radically operated (R0) and monitored in 1975-2022 (m=558, f=241; total gastrectomies=173, distal gastrectomies=461; proximal gastrectomies=165; combined gastrectomies=247 with resection of esophagus, pancreas, liver, duodenum, diaphragm, colon transversum, splenectomy, etc; only surgery-S=624, adjuvant chemoimmunotherapy-AT=175 (5-FU + thymalin/taktivin); T1=238, T2=220, T3=184, T4=157; N0=437, N1=109, N2=253, M0=799; G1=222, G2=164, G3=413. Variables selected for prognosis study were input levels of 45 blood parameters, sex, age, TNMG, cell type, tumor size. Survival curves were estimated by the Kaplan-Meier method. Differences in curves between groups of GCP were evaluated using a log-rank test. Multivariate Cox modeling, discriminant analysis, clustering, SEPATH, Monte Carlo, bootstrap and neural networks computing were used to determine any significant dependence. RESULTS: Overall life span (LS) was 2128.9±2300.3 days and cumulative 5-year survival (5YS) reached 58.4%, 10 years – 51.9%, 20 years – 39%, 30 years – 27.2%. 318 GCP lived more than 5 years (LS=4304.5±2290.6 days), 169 ECP – more than 10 years (LS=5919.5±2020 days). 290 GCP died because of GC (LS=651±347.2 days). Cox modeling displayed that ECP survival significantly depended on CRF: healthy cells/CC, erythrocytes/CC, monocytes/CC, phase transition (PT) in terms of synergetics early— invasive cancer; PT N0--N12, age, G1-3, hemorrhage time, ESS, sex, AT, prothrombin index, residual nitrogen. Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early—invasive cancer (rank=1); PT N0--N12 (2); healthy cells/CC (3), erythrocytes/CC (4), thrombocytes/CC (5), monocytes/CC (6), segmented neutrophils/CC (7), leucocytes/CC (8), lymphocytes/CC (9), stick neutrophils/CC (10), eosinophils/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0). CONCLUSIONS: GCP survival after radical procedures significantly depended on CRF. Cox Proportional Hazards Results, n=799 Parameter Estimate Standard Error Chi- square P value 95% Lower CL 95% Upper CL Hazard Ratio ESS -0.012083 0.004865 6.16915 0.013000 -0.021618 -0.002548 0.987990 Hemorrhage Time 0.001295 0.000371 12.20046 0.000478 0.000568 0.002021 1.001296 Residual Nitrogen 0.049233 0.008903 30.58332 0.000000 0.031784 0.066681 1.050465 Prothrombin Idex 0.021321 0.004897 18.95581 0.000013 0.011723 0.030920 1.021550 Age 0.012628 0.006097 4.28971 0.038344 0.000678 0.024577 1.012708 Sex 0.304544 0.122528 6.17776 0.012937 0.064394 0.544694 1.356006 G1-3 0.163023 0.065880 6.12346 0.013340 0.033902 0.292145 1.177064 Procedure Type 0.229288 0.072502 10.00130 0.001564 0.087186 0.371390 1.257704 Adjuvant Treatment -0.518082 0.177398 8.52903 0.003495 -0.865775 -0.170388 0.595662 PhT Early-Invasive Cancer 1.282134 0.239070 28.76183 0.000000 0.813565 1.750703 3.604323 PhT N0---N12 0.453418 0.066399 46.63044 0.000000 0.323278 0.583559 1.573682 Cox Regression B SE Wald df P Exp(B) 95,0% CI Lower Upper Erythrocytes/CC ,089 ,039 5,331 1 ,021 1,093 1,014 1,179 Monocytes/CC ,213 ,100 4,548 1 ,033 1,237 1,017 1,505 Healthy Cells/CC -,043 ,012 12,956 1 ,000 ,958 ,936 ,981 Survival Function GCP=799; 5YS=58.4%; 10YS=52.2%; 20YS=40.3%; 30YS=27.2%. Complete Censored -5 0 5 10 15 20 25 30 35 40 Years after Gastrectomies 0,1 0,2 0,3 0,4 0,5 0,6 0,7 0,8 0,9 1,0 Cumulative Proportion Surviving Cumulative Proportion Surviving (Kaplan-Meier) Complete Censored 10-Year Survival of Early GCP=88.4%; 10-Year Survival of Invasive GCP=41.5%; P=0.000 by Log Rank Test. 0 5 10 15 20 25 30 35 Years after Gastrectomies 0,3 0,4 0,5 0,6 0,7 0,8 0,9 1,0 Cumulative Proportion Surviving Invasive GCP Early GCP Cumulative Proportion Surviving (Kaplan-Meier) Complete Censored 10-Year survival GCP N0=69.7%; 10-Year Survival GCP N1-2=29.5%; P=0.000 by Log Rank. 0 5 10 15 20 25 30 35 40 Years after Gastrectomies 0,0 0,1 0,2 0,3 0,4 0,5 0,6 0,7 0,8 0,9 1,0 Cumulative Proportion Surviving GCP N1-2 GCP N0 Cumulative Proportion Surviving (Kaplan-Meier) 10-Year Survival GCP after AT=59.7%; 10-Year Survival after Surgery=50.6%; P=0.032 by Log Rank Test. Complete Censored 0 5 10 15 20 25 30 Years after Gastrectomies 0,1 0,2 0,3 0,4 0,5 0,6 0,7 0,8 Cumulative Proportion Surviving only Surgery AT Neural Networks: n=611; Baseline Error=0.000; Area under ROC Curve=1.000; Correct Classification Rate=100% Rank Sensitivity Phase Transition Early-Invasive Cancer 1 58263 Phase Transition N0—N12 2 51328 Healthy Cells/Cancer Cells 3 33644 Erythrocytes/Cancer Cells Thrombocytes/Cancer Cells Monocytes/Cancer Cells Segmented Neutrophils/Cancer Cells Leucocytes/Cancer Cells Lymphocytes/Cancer Cells 4 5 6 7 8 9 25968 20448 12218 13604 12400 10482 Stick Neutrophils/Cancer Cells Eosinophils/Cancer Cells 10 11 10002 8630